
Translate this page into:
Arthroscopic management of synovial chondromatosis of the shoulder: A case report
*Corresponding author: Shwetank Gangwar, Department of Orthopaedic Surgery, Sir Ganga Ram Hospital, New Delhi, India. shwetank.gangwar25@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Gangwar S, Singh A, Bhasin VB. Arthroscopic management of synovial chondromatosis of the shoulder: A case report. J Arthrosc Surg Sports Med 2022;3:53-6.
Abstract
Synovial chondromatosis of the shoulder is a rare entity that is generally mono-articular and uncommon in diarthrodial joints. Treatment of synovial chondromatosis of the shoulder includes open arthrotomy retrieval of loose bodies and synovectomy. With advances in arthroscopy, the same could be achieved using arthroscopic techniques. This case report describes a case report of a 35-year-old male patient who presented with complaints of pain and restriction of movement for 6 months. The MRI of the patient was suggestive of multiple loose bodies in the shoulder joint, in the subdeltoid region, and subscapularis muscle with subacromial bursitis. Arthroscopically more than 100 loose bodies were retrieved with subacromial decompression. Shoulder synovial chondromatosis has been rarely reported in the literature. The malignant transformation although rare, but it is still a possibility. The recurrence rate varies from 3.2% to 22.3%. Open arthrotomy, synovectomy, and retrieval of loose bodies cause delayed recovery and more morbidity with high chances of subscapularis insufficiency due to the need of subscapularis tenotomy. Arthroscopic treatment although have limitations such as limited visualization, limited synovectomy, and difficult interventions around the axillary recess or biceps sheath, but provides with the advantage of lesser morbidity and early rehabilitation. Synovial chondromatosis can be successfully treated arthroscopically as it provides intra-articular and extra articular access with early rehabilitation, lesser morbidity, and early recovery.
Keywords
Arthroscopic management
Loose bodies
Shoulder synovial chondromatosis
Subacromial bursitis

INTRODUCTION
Synovial chondromatosis is condition where there is the proliferation of the synovial membrane and metaplasia, with the development of multiple cartilaginous or osteocartilaginous nodules within the joint, bursa, or tendinous sheath.[1] It is a mono-articular arthropathy that is rarely seen in the diarthrodial joints. Its etiology is unknown, although it has been associated with chromosomal mutations (p21.3 and 12q13) that affect proteins.[2] Knee joint is the primary site of involvement followed less commonly by hip, elbow, ankle, temporomandibular, and shoulder joints respectively.[3,4] It occurs most often in those aged 30–50 years and 3 times more in males than females.[5] Although the reasons for the development of synovial chondromatosis are not known, it has been suggested that in the pathogenesis, the synovial chondroid metaplastic focus becomes peduncular then by breaking off, becomes a free fragment within the joint. These free fragments may undergo endochondral ossification or cause erosive damage to the joint surface.[6]
The treatment for synovial chondromatosis in the past has classically been open arthrotomy, synovectomy, and removal of the free fragments. With recent advances in arthroscopic techniques, arthroscopy has become one of the methods for treatment of synovial chondromatosis of the shoulder. Arthroscopy of the shoulder is not only an extremely skilled surgery but also requires a lot of perseverance and patience when it comes to technically challenging procedures such as retrieval of multiple loose bodies of varying sizes. Arthroscopic treatment of the pathologies is associated with reduced morbidity and early mobilization of the shoulder joint.
CASE PRESENTATION
A 35-year-old male patient, an IT professional presented with complaints of left shoulder pain and restriction of movement for 6 months. The pain was insidious in onset, gradually progressive, dull aching, non-radiating, aggravated with shoulder movements which decreased with taking rest or medication with no diurnal variation. The patient was treated conservatively with medications. The patient was unable to comb hair, reach for overhead objects, and he had difficulty in riding his motor bike. There was no history of trauma, fever, multiple joint pains, and morning stiffness of joints, no loss of weight or appetite, or any other systemic illness.
On physical examination, there was muscle wasting. There was no local rise of temperature or tenderness. His range of movements was grossly restricted with flexion of 45 degrees, extension of 10 degrees, abduction of 30 degrees, external rotation of 30 degrees, and internal rotation of 15 degrees. The shoulder movements were associated with pain and crepitus. There was no distal neurovascular deficit. The contra-lateral shoulder joint and other joints examination were normal. The general systemic and physical examination was normal.
The hemogram, erythrocyte sedimentation rate, C-reactive protein were normal. The X-ray [Figure 1] showed multiple loose bodies in the shoulder joint. The MRI [Figure 2] showed multiple loose bodies in the shoulder joint, in the subdeltoid region, and subscapularis muscle with subacromial bursitis. The patient was then prepared for arthroscopic removal of the loose bodies and subacromial decompression with informed written consent. The patient was made to lie in the beach chair position under general anesthesia. Posterior, posterolateral and anterior portals were used for the procedure. Most of the loose bodies were extracted through the anterior portal. The loose body extraction was followed by subacromial decompression. More than a 100 loose bodies [Figures 3-5] of varying size and shapes were removed arthroscopically. The patient was given arm pouch post-operatively. The patients shoulder was mobilized both actively and passively on the 4th post-operative day after the patient was comfortable enough to initiate shoulder movements.
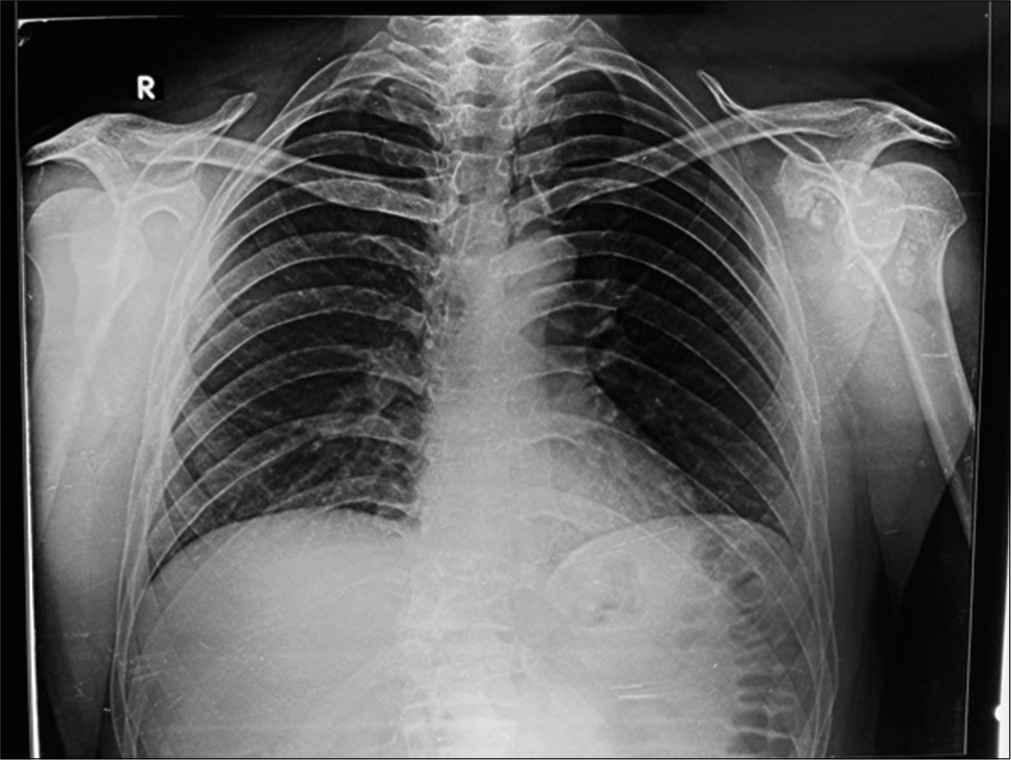
- Pre-operative x-ray showing multiple loose bodies in the left shoulder.
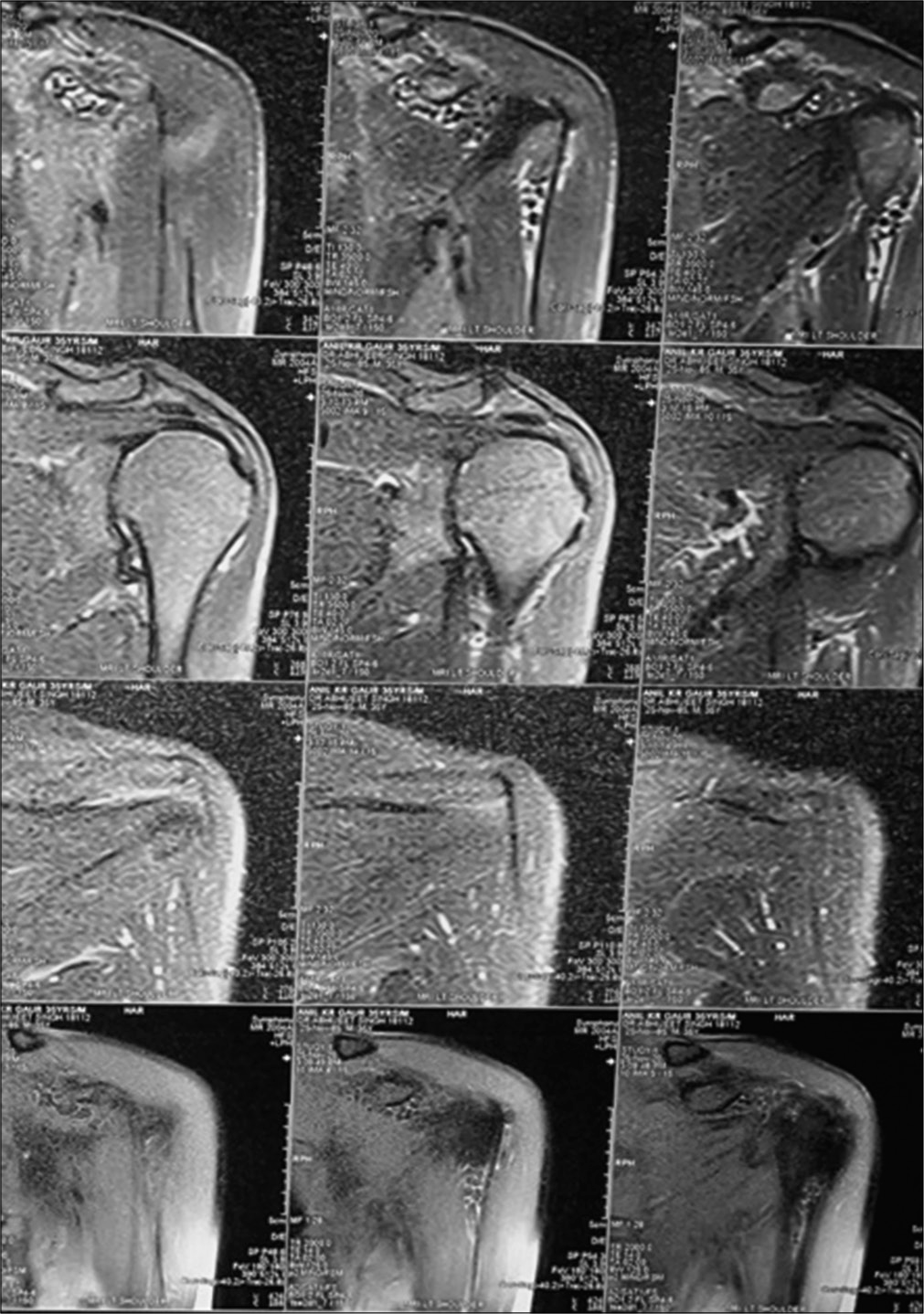
- MRI of the left shoulder showing multiple loose bodies.
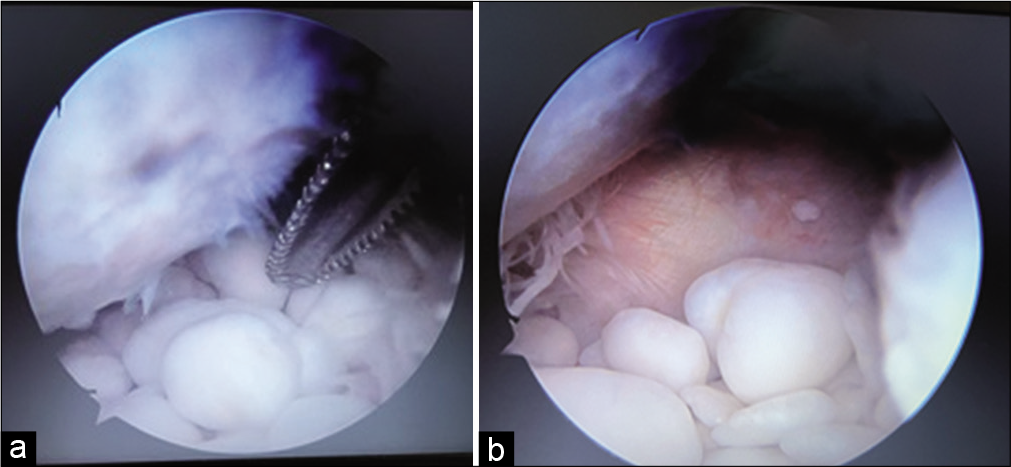
- (a and b) Multiple loose bodies in the shoulder joint.
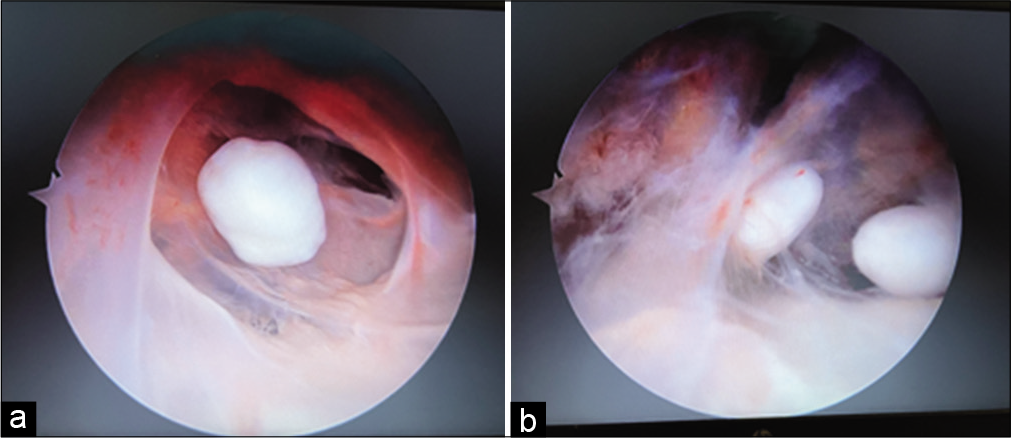
- (a and b) Multiple loose bodies inside the subscapularis muscle belly.

- Over a 100 loose bodies of varying size and shape were removed.
DISCUSSION
The case of synovial chondromatosis of the shoulder is very uncommon and its arthroscopic treatment has not been studies much in the literature. The recurrence rate of synovial chondromatosis ranges from 3.2% to 22.3%.[7] Although the disease is quite uncommon, it still displays the possibility of malignant transformation. Recurrent synovial chondromatosis at the same location favors diagnosis malignant transformation to synovial chondrosarcoma.[8]
Although the definitive etiology of synovial chondromatosis is not known, it can be classified as primary or secondary. The primary form is uncommon, it does not have a known cause and is frequently monoarticular. Secondary reasons include primarily trauma, then osteochondritis dissecans, rheumatoid arthritis, and tubercular arthritis. Milgram defined three stages of synovial chondromatosis. At Stage 1, there is active intrasynovial disease but no free fragments. At Stage 2, there is active intrasynovial proliferation, and lesions are seen in transition to free fragments, and at Stage 3, there are multiple osteochondral free fragments, but active intrasynovial disease is not seen.[9]
Controversy still lies over the management, whether open removal of the loose bodies is better or the arthroscopic retrieval is better. Open surgery would provide easy access to sites that would be difficult with arthroscopy, wide visualization capability.[10,11] However, mandatory subscapularis tenotomy, higher morbidity, and inhibition of early rehabilitation are the main disadvantages of open surgery.[5] Arthroscopy allows to avoid damaging the subscapularis and does not require dissection of tissues, improving the Constant test significantly according to Lunn (P < 0.04), without significant restrictions on mobility and a more satisfactory postoperative stage.[12] Main disadvantages of arthroscopic surgery are permission of limited synovectomy and difficult interventions around the axillary recess or biceps sheath.[11] There might be a need to change portals of the scope and suction cannula to remove loose bodies in different joint spaces. The subacromial space must be looked for loose bodies. Thorough cleaning, lavage, and synovectomy are important parts of this surgery.[13]
CONCLUSION
Arthroscopic treatment of the synovial chondromatosis of the shoulder is recommended in patients because it provides intra-articular and extra-articular access with early rehabilitation, lesser morbidity, and early recovery.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Nonseptic monoarthritis: Imaging features with clinical and histopathologic correlation. Radiographics. 2000;20:S263-78.
- [CrossRef] [PubMed] [Google Scholar]
- Arthroscopic treatment of synovial chondromatosis, an unusual cause of shoulder pain. Reumatol Clin. 2014;10:416-7.
- [CrossRef] [PubMed] [Google Scholar]
- Primary synovial chondromatosis of the shoulder: Clinical, arthroscopic and histopathological aspects. Knee Surg Sports Traumatol Arthrosc. 2005;13:483-8.
- [CrossRef] [PubMed] [Google Scholar]
- Operative treatment of primary synovial osteochondromatosis of the hip: Surgical technique. J Bone Joint Surg. 2007;89:232-45.
- [CrossRef] [Google Scholar]
- Arthroscopic treatment of synovial chondromatosis of the shoulder: Report of three patients. J Shoulder Elbow Surg. 2009;18:e4-8.
- [CrossRef] [PubMed] [Google Scholar]
- Arthroscopic treatment for synovial chondromatosis of the shoulder. Arthroscopy. 2003;19:E2.
- [CrossRef] [PubMed] [Google Scholar]
- Primary synovialchondromatosis: A clinicopathologic review and assessmentof malignant potential. Hum Pathol. 1998;29:683-8.
- [CrossRef] [Google Scholar]
- Synovial chondromatosis and chondrosarcdoma. A study of the relationship between these two disease. Rev Chir Orthop Reparatrice Appar Mot. 1996;82:216-24.
- [Google Scholar]
- Synovial osteochondromatosis: A histological study of thirty cases. J Bone Joint Surg Am. 1977;59:792-801.
- [CrossRef] [PubMed] [Google Scholar]
- Synovial chondromatosis of the shoulder: Open synovectomy and insertion of osteoarticular allogaft with internal fixation to repair intraoperative glenohumeral joint instability. Am J Orthop (Belle Mead NJ). 2011;40:E154-8.
- [Google Scholar]
- Synovial chondromatosis of the glenohumeral joint: A rare condition. Arch Orthop Trauma Surg. 2001;121:109-11.
- [CrossRef] [PubMed] [Google Scholar]
- Arthroscopic synovectomy, removal of loose bodies and selective biceps tenodesis for synovial chondromatosis of the shoulder. J Bone Joint Surg Br. 2007;89:1329-35.
- [CrossRef] [PubMed] [Google Scholar]
- Shoulder rheumatoid arthritis associated with chondromatosis, treated by arthroscopy. Arthroscopy. 1991;7:233-6.
- [CrossRef] [Google Scholar]




