
Translate this page into:
Intra-articular lipoma of the hip joint – A report of two cases and literature review
 , Vijay Ram Kumar Papineni4, Rajesh Botchu2,
, Vijay Ram Kumar Papineni4, Rajesh Botchu2,
*Corresponding author: Rajesh Botchu, Department of Musculoskeletal Radiology, Royal Orthopedic Hospital, Birmingham, United Kingdom drrajeshb@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Mettu S, Gavvala SN, Iyengar KP, Papineni VR, Botchu R. Intra-articular lipoma of the hip joint – A report of two cases and literature review. J Arthrosc Surg Sports Med. 2025;6:74-7. doi: 10.25259/JASSM_24_2024
Abstract
Intra-articular lipoma of the hip joint is a rare entity with a mere 4 cases being reported to date We present two patients with true intra-articular hip lipomas, with insidious onset of non-traumatic hip pain and gradual restriction in the range of motion. Magnetic Resonance Imaging (MRI) revealed an encapsulated intra-articular lesion with the typical imaging characteristics of a benign lipomatous tumour and a similar signal as that of fat tissue.. Arthroscopic excision of the intra-articular lipoma was done in one patient. An intra-articular lipoma is a rare synovial tumour of the hip joint with typical imaging characteristics and this article highlights clinical presentation, radiological features, and management options.
Keywords
Lipoma
Intra-articular
Hip joint
Orthopedics
Musculoskeletal
Synovial joint disorders
Magnetic resonance imaging

INTRODUCTION
Lipomas are among the most common soft-tissue tumors in our daily clinical practice. However, intra-articular lipomas are a rare entity. A literature search revealed 35 cases of true intra-articular (synovial) lipoma involving knee, hip, tarsometatarsal, and elbow and shoulder joints. Those involving the hip joint are very uncommon. In this article, we report two cases of intra-articular lipoma of the hip joint. Lipomas comprise mature fat classified as superficial or deep, single or multiple lipomas. They present clinically with symptoms of mass effect, most commonly pain and limited range of movement. Till now, only four cases of intra-articular lipoma of the hip have been reported in the literature. The common sites in the hip joint are the cotyloid fossa of the acetabulum, the anterior and posteroinferior aspects of the femoral neck, and the posterior aspect of the femoral head.[1-3] Other reported symptoms include prolonged standing pain, swelling, and discomfort. Most of these patients present with gradually worsening pain and locking during weight-bearing or hip flexion. The signs usually elicited include decreased range of motion and evidence of impingement but with a soft endpoint.
Initial plain radiographs may reveal lucent regions, especially when these intra-articular lipomas are large. On computed tomography, these lesions appear as fat-density lesions. An ultrasound reveals them as round, homogenously hyperechoic intra-articular lesions with no internal vascularity. Magnetic resonance imaging (MRI) is the gold standard investigation with T1 and T2 homogenously hyperintense signal suppressing on short-tau inversion recovery (STIR) sequences.
Management is surgical in patients with symptomatic lesions. At present, there is a paucity of information about the conservative management of such intra-articular lesions. Arthroscopic excision provides the least intrusive management of intra-articular lipomas of the hip joint, though complications such as stiffness and keloid formation have been reported. There is a lack of substantial data regarding recurrence or specific complications, and future longitudinal studies would substantiate a more detailed understanding of this condition.
CASE REPORTS
Case 1
A 34-year-old male presented with vague and insidious-onset left hip pain. It gradually worsened for over a year. There was no documented history of antecedent trauma to the left hip, and the patient was systemically well with no underlying general disease. On physical examination, there was a restriction in the range of motion with occasional clicking symptoms. The neurovascular examination was normal. Hematological investigations did not reveal anything significant to explain the symptoms. An initial radiograph of the hip joint did not show any significant pathology. On MRI, the lesion appeared as an ovoid intra-articular homogenous T1 and T2 hyperintense lesion with complete fat suppression on STIR images along the posterior aspect of the femoral neck. There was no calcification or fat necrosis. These imaging findings were characteristic of an intra-articular lipoma of the hip joint [Figure 1]. The differential diagnosis was Lipoma arborescence with finger-like projections and pigmented villonodular synovitis (PVNS) (Dark on T1T2). The patient subsequently underwent an arthroscopic excision of the mass. The post-operative period was uneventful, and the range of motion gradually improved during the routine follow-up examinations.
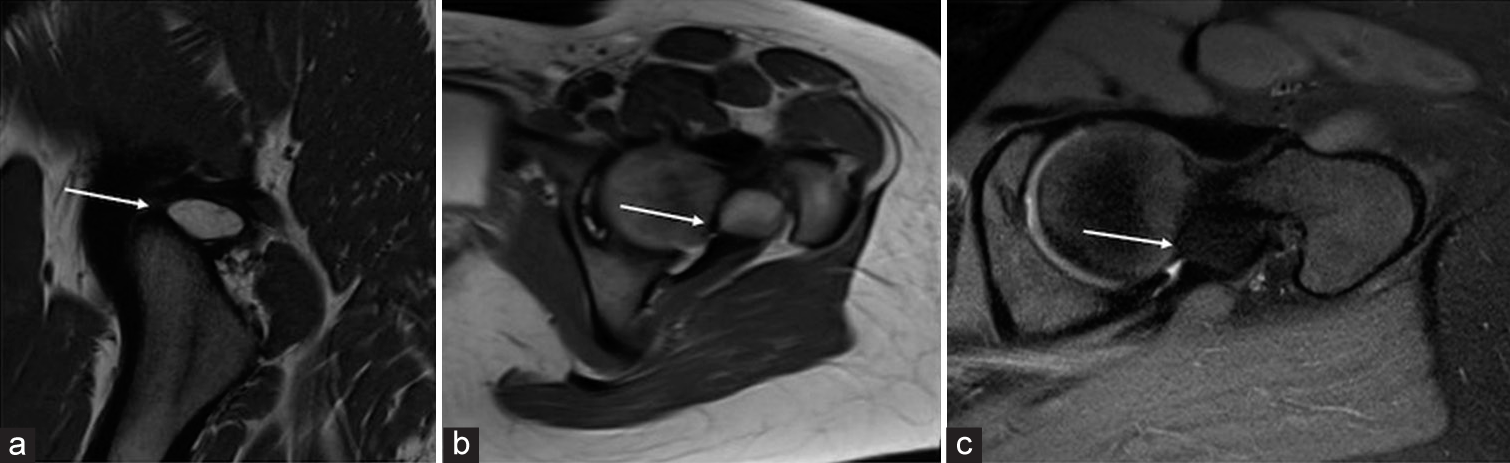
- (a) Sagittal T1 and (b) axial T2 images show a centimetric, well-defined solitary ovoid intra-articular mass (white arrows) along the posterior aspect of the femoral neck. (c) The lesion was homogenously hyperintense on T1-weighted and T2-weighted images with complete fat suppression on short-tau inversion recovery images (white arrow). The lesion follows the subcutaneous fat signal on all sequences.
Case 2
A 19-year-old male presented to the orthopedic clinic with complaints of insidious onset right hip pain over the past 10 years with partial restriction of movements. He denied any history of trauma or known systemic joint disorder. His gait appeared satisfactory. On physical examination, there was a global restriction in the range of motion of the right hip joint compared to the opposite side. The neurovascular status was intact. Hematological investigations did not reveal anything significant to explain the patient’s symptoms. A radiograph of the right hip joint was normal. On MRI, the lesion appeared as an ovoid homogenous and T2 hyperintense lesion completely suppressing on STIR along the inferior margin of the femoral neck. No evidence of calcification, necrosis, or non-lipomatous component was noted. These imaging findings were characteristic of an intra-articular lipoma of the hip joint [Figure 2]. Surgical excision was advised for this; however, the patient did not proceed with the same. The patient seemed reassured after being explained the nature of the pathology. In the interim, it was advised that he initiated a follow-up; that is, he was encouraged to review if he became further symptomatic and the condition started to affect his activities of daily living.
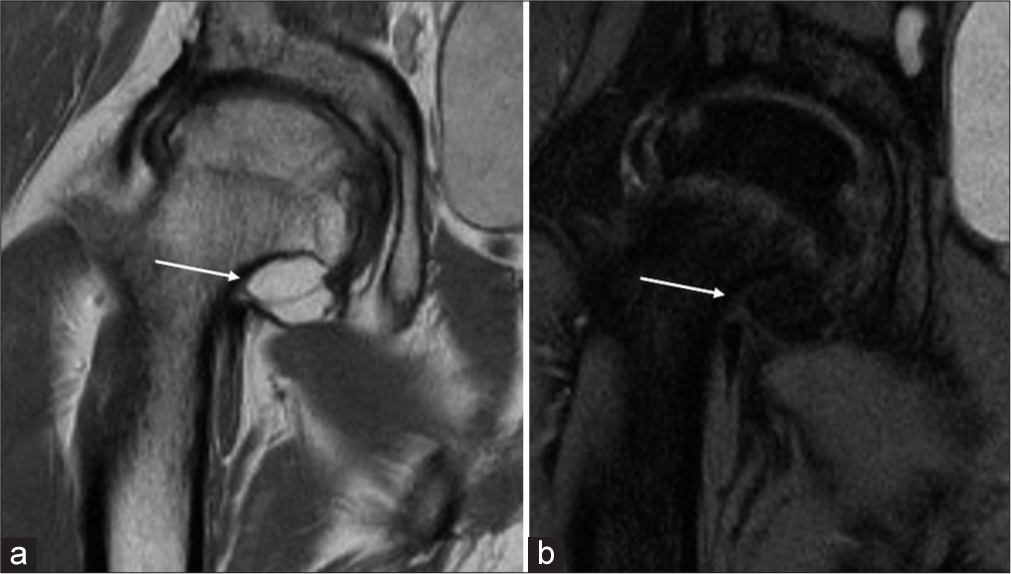
- (a) Coronal T2 and (b) short-tau inversion recovery images show a centimetric intra-articular mass along the inferior margin of the femoral neck (white arrows).
DISCUSSION
Less than 1% of lipomas are intra-articular, an uncommon type of lipoma that usually develops inside a joint. Intra-articular lipoma most frequently develops in the knee joint, although it can also affect other joints, notably the hip, shoulder, and spine, in descending order of prevalence.[4-7] The existing literature has documented four instances of intra-articular lipoma affecting the hip joint.[1-3] Along the cotyloid fossa of the acetabulum,[2] the anterior[2] and posteroinferior aspects of the femoral neck[1] and the posterior aspect of the femoral head were the typical locations described in these articles. Previous cases showed that synovial lipomas in the hip joint caused insidious onset pain with gradual worsening and episodic mechanical symptoms due to mass effect or mechanical joint locking during weight-bearing or hip flexion. Torsion of the lipoma stalk and formation of loose bodies were seen in some of the knee joint intra-articular lipomas.[7,8]
In addition to our cases, all the above hip cases did not show anything significant on initial radiographs. They showed a characteristic appearance on MRI as small solid, well-circumscribed homogenous T1 and T2 hyperintense mass with uniform fat suppression on STIR or fat suppression sequences. Most intra-articular lipomas were excised, addressing any concomitant acetabular labral tears if present.[2,3] Surgical excision is recommended in most cases as the presence of intra-articular lipoma changes the biomechanical axis with mechanical overloading of the femoral head and acetabulum, resulting in accelerated unilateral asymmetric hip osteoarthritis.[1,9-11]
The most common differentials for intra-articular fat-containing lesions include benign lesions such as lipoma arborescence, synovial osteochondromatosis, PVNS, hemangioma, liposarcoma, and intra-articular lipoma.[1]
Diagnosing and characterizing the intra-articular masses based on imaging findings may be crucial, as treatment options and prognosis vary depending on the disease. Each pathology has distinct radiologic characteristics that set them apart from intra-articular synovial lipoma and one another. It is crucial to distinguish intra-articular synovial lipoma from its more common mimic, lipoma arborescence. It appears as a frond-like fatty mass with multiple villous projections of fatty synovial tissue within the joint.[12] Conversely, intraarticular synovial lipoma usually presents as a solitary well-circumscribed lobulated or pedunculated fatty mass.
Synovial osteochondromatosis shows characteristic multiple cartilaginous loose bodies that proliferate and erode adjacent bones or display early osteoarthritic changes.[13] Meanwhile, focal or diffuse nodular synovitis (PVNS) demonstrates dark signal intensity on all MRI pulse sequences.[14] Synovial hemangioma is characterized by a multilobulated intra-articular mass with marked T2-weighted (T2-w) hyperintensity due to intralesional vascular pooling.[15]
Although chondrolipoma and osteochondroid metaplasia have been reported in the knee joint, there is a lack of published research describing a similar lipoma variant in the hip joint.
In rare cases, joint-based malignancies such as synovial metastases, synovial sarcoma, or synovial chondrosarcoma have been diagnosed in isolated cases.[16-18] De-differentiation of intraarticular synovial lipoma into liposarcoma is a dreaded but well-documented possibility.[6,8] It is vital to consider intra-articular malignancies in the differential diagnosis, and they demonstrate iso- or hypointense T1-weighted and heterogeneous T2-weighted signals, distinguishing them from synovial lipoma. Aggressive imaging features such as surrounding soft-tissue extension, bony erosions, and destruction of joint space are also seen as malignant rather than benign pathologies.
CONCLUSION
Intra-articular lipomas are uncommon synovial tumors affecting the hip joint with a discernible radiological appearance. The medical literature only contains a restricted number of documented cases of these conditions. These cases emphasize the significance of MRI for precise diagnosis and the necessity for increased awareness among musculoskeletal radiologists and orthopedic surgeons. Radiologists must know the distinctive features that distinguish true intraarticular lipomas from other fat-containing lesions. A close collaboration between clinicians and radiologists is essential to improve patient outcomes through timely diagnosis and appropriate management.
Author contributions
SM, RB: Conception and design, or acquisition of data, or analysis and interpretation of data; SM, KPI, VRKP, RB: Design, or acquisition of data, or analysis and interpretation of data; SM, SN, KPI, VRKP, RB: drafting the article or revising it critically for important intellectual content, and final approval of the version to be published.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- An intra-articular synovial lipoma of the hip, possibly causing osteoarthritis: A case report and review of the literature. Skeletal Radiol. 2018;47:717-21.
- [CrossRef] [Google Scholar]
- Intra-articular lipoma of the hip. A case report. Int Orthop. 1998;22:328-9.
- [CrossRef] [Google Scholar]
- Intra-articular lipoma of the hip. BMJ Case Rep. 2017;2017:bcr2017220349.
- [CrossRef] [Google Scholar]
- Large intra-articular true lipoma of the knee. BMC Musculoskelet Disord. 2019;20:110.
- [CrossRef] [Google Scholar]
- Intra-articular synovial lipoma in the posteromedial compartment of the knee. Arthrosc Orthop Sports Med. 2014;1:54-8.
- [CrossRef] [Google Scholar]
- Intra-articular synovial lipoma of the knee joint (located in the lateral recess): A case report and review of the literature. Knee. 2007;14:63-7.
- [CrossRef] [Google Scholar]
- Knee locking in osteoarthritis due to synovial lipoma: A case report. J Clin Diagn Res. 2013;7:1708-9.
- [CrossRef] [Google Scholar]
- Torsion of an intra-articular lipoma as a cause of pseudo-locking of the knee. Arthroscopy. 2003;19:E27.
- [CrossRef] [Google Scholar]
- Early MRI findings of rapidly destructive coxarthrosis. Skelet Radiol. 2002;31:35-8.
- [CrossRef] [Google Scholar]
- Early MRI and intraoperative findings in rapidly destructive osteoarthritis of the hip: A case report. Int J Surg Case Rep. 2015;8:13-7.
- [CrossRef] [Google Scholar]
- The acetabular rim syndrome. A clinical presentation of dysplasia of the hip. J Bone Joint Surg (Br). 1991;73:423-9.
- [CrossRef] [Google Scholar]
- MR imaging of lipoma arborescens and the associated lesions. Skelet Radiol. 2003;32:504-9.
- [CrossRef] [Google Scholar]
- MR appearance of idiopathic synovial osteochondromatosis. J Comput Assist Tomogr. 1993;17:772-6.
- [CrossRef] [Google Scholar]
- Pigmented villonodular synovitis: MRI characteristics. Skelet Radiol. 1995;24:7-12.
- [CrossRef] [Google Scholar]
- Synovial hemangioma: Imaging features in eight histologically proven cases review of the literature, and differential diagnosis. Skelet Radiol. 1995;24:583-90.
- [CrossRef] [Google Scholar]
- MRI features of three paediatric intra-articular synovial lesions: A comparative study. Clin Radiol. 2008;63:805-12.
- [CrossRef] [Google Scholar]
- Primary synovial chondromatosis of the hip joint (PrSC of the hip): A retrospective cohort analysis and review of the literature. J Clin Orthop Trauma. 2022;35:102068.
- [CrossRef] [Google Scholar]




