
Translate this page into:
Translate and cross-culturally adapt the original English version of the lower extremity functional scale into the Sinhalese version
*Corresponding author: Sanka Theekshana Thebuwanaarachchi, Sports Medicine Unit, Teaching Hospital Karapitiya, Galle, Sri Lanka. sankatheekshana@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Thebuwanaarachchi ST. Translate and cross-culturally adapt the original English version of the lower extremity functional scale into the Sinhalese version. J Arthrosc Surg Sports Med. 2025;6:43-53. doi: 10.25259/JASSM_39_2024
Abstract
Objectives:
Functional ability is critical for quality of life (QOF), and its evaluation is vital in a clinical context. However, there is a deficiency of a universally recognized grading scale in Sinhala for assessing functional capacity in athletes with lower extremity musculoskeletal conditions. This research aimed to validate the linguistic and cross-cultural adaptation of a translated Sinhala version of the lower extremity functional scale (S-LEFS).
Materials and Methods:
A two-stage observational study was conducted. The lower extremity functional scale was cross-culturally adapted to Sinhala through independent, double forward, and backward translation. An experienced clinical researcher tested the translated version to establish the linguistic validation of S-LEFS. The finalized version was validated for construct, convergent, and criterion validity. A total of 112 participants, comprising 57 healthy (50.89%) and 55 unhealthy (49.11%) lower limb athletes, completed S-LEFS.
Results:
S-LEFS demonstrated excellent reliability with a Cronbach’s alpha of 0.952. Exploratory factor analysis revealed good factor loadings (>0.48) for all 20 items, with three components accounting for 70.63% of cumulative variance. Scale got a sensitivity of 87.5% and specificity of 81% at a cutoff point of 67.5. Kaiser-Meyer-Olkin (KMO) value was 0.918 (P < 0.0001), and Bartlett’s Test of Sphericity was significant (P < 0.01). No correlation was detected between S-LEFS and World Health Organization QOF-Bref (r = 0.281).
Conclusion:
S-LEFS is a reliable and valid tool for evaluating lower limb function in athletes.
Keywords
Lower extremity functional scale
Sinhala version of the lower extremity functional scale
World Health Organization quality of life-bref
Translation
Validation

INTRODUCTION
The complementary tomography, physical examination, and clinical evaluation are thought inadequate to establish the level of function of an individual, especially an athlete, after injury or surgery.[1] Precise functional assessment has been demonstrated and proven evidently to be effective in rehabilitation and administering treatment primarily focused on individual disabilities rather than relying merely on clinical assessments derived from diagnostic tests.[2] Assessing patients’ and athletes’ awareness of their quality of life (QOF), along with monitoring enhancements in their clinical and functional status, is substantially becoming a standard practice in both, scientific and clinical societies.[3,4] Physical function is commonly assessed through patient-reported measures such as the Western Ontario and McMaster Universities Arthritis Index (WOMAC), hip disability, and osteoarthritis outcome score (HOOS), EuroQol- 5 Dimension (EQ-5D), and 36-Item Short Form Survey (SF-36). The WOMAC primarily focuses on pain, symptoms, and daily activities in individuals with hip osteoarthritis, while the HOOS expands on this by including sub-scales for recreation and sports.[5,6] The EQ-5D and SF-36 provide broader health assessments, with the SF-36 covering eight distinct sub-scales.[7,8] Despite extensive research, no standard tool has been established to accurately predict post-operative outcomes for patients undergoing lower limb surgeries or rehabilitation outcomes following treating athletes with lower limb injuries.[9,10]
The lower extremity functional scale (LEFS), developed by Binkley et al.. in 1999[11] is extensively used to assess lower limb function. It is a straightforward, user-friendly tool designed according to a model proposed by the World Health Organization.[12]
LEFS offers excellent test-retest reliability (R = 0.94) and greater sensitivity to change compared to the SF-36, particularly in total joint patients. These attributes make the LEFS exceptionally superior for precisely tracking recovery and effectively setting goals in physical therapy, as well as a more efficient and suitable tool for thoroughly assessing lower extremity musculoskeletal issues compared to other commonly used measures.[11] This is precisely why LEFS is deliberately chosen over other tools.
The original LEFS, developed and published in English, was designed to evaluate the functional status and level of athletes with musculoskeletal disorders in the lower limbs. It comprises 20 questions, each offering 5 numeric response options from 0 to 4, leading to an overall score that ranges from 0 (poor) to 80 (excellent). The LEFS has demonstrated outstanding reliability and responsiveness.[13-15] However, before a questionnaire can be employed in a different language, it is essential for it to be translated and culturally adapted to the specific country where it will be applied.[16,17] It is worth noting that, in comparison to the SF-36, the LEFS has demonstrated to have exceptional psychometric properties. After its establishment, the LEFS was culturally adapted and translated from its original English version into various languages worldwide, including German,[12] Italian,[18] Dutch,[19] Persian,[20] Brazilian Portuguese,[21] Greek,[22] and Malaysian[23]
In each of these adaptations, the LEFS has consistently maintained a strong psychometric profile, demonstrating excellent reliability and validity. This makes the LEFS a reliable and trustworthy instrument for evaluating lower limb function in patients with musculoskeletal dysfunction across different cultures and languages ensuring its efficacy in various clinical and research environments worldwide. Translating and adapting the LEFS into Sinhala can profoundly impact rehabilitation and clinical practice in Sri Lanka. It would make functional assessments more accessible and culturally relevant, improving patient understanding and communication with healthcare providers. This enhances the accuracy of assessments and the effectiveness of personalized treatment plans. Standardizing the LEFS in Sinhala would enable consistent, comparable data collection across the country, aiding in better patient outcome tracking and local research. Ultimately, it empowers healthcare providers, improves treatment outcomes, and contributes to developing culturally appropriate rehabilitation practices and policies in Sri Lanka.
This study aimed to translate the LEFS into Sinhala and validate it through various procedures, including construct validity applying exploratory factor analysis, convergent validity assessed by Pearson’s correlation coefficient, and criterion validity through the gold standard method. This research addresses several significant gaps. First, there is a lack of a validated scale in Sinhala, highlighting the necessity for its development. Second, the study sought to establish an appropriate cutoff point for Sri Lankan athletes by creating a Sinhala version of the LEFS that retains the excellent psychometric properties, reliability, and validity of the original form, thus ensuring its suitability for use with Sri Lankan athletes.
MATERIALS AND METHODS
The accepted method for translating and validating a questionnaire involved several steps: Translating the questionnaire, establishing linguistic and face validity, and assessing internal consistency through Cronbach’s alpha. Principal component analysis was conducted in this study to explore underlying factors, with factor analysis helping to understand how factor loadings correspond to meaningful themes, particularly in the newly translated questionnaire. For factor analysis, the sample size needed to include at least five participants per item in the questionnaire, as recommended by Mapi research trust guidelines. In addition, the specificity and sensitivity of the questionnaire were calculated.
This study was conducted as an observational study in two stages. Stage one began with the preliminary Sinhala translation and cross-cultural adaptation of the LEFS. In the second stage, a prospective evaluation of the critical psychometric properties of the Sinhala version of the LEFS was conducted.
The Ethics Review Committee of the University of Ruhuna granted the authorization for this study, and all participating athletes offered their written informed consent. In addition, the research and publication of the conclusions were granted by the copyright holder of the original LEFS.
Translation procedure
The LEFS was translated from its original English version to the Sinhalese version according to the forward/backward translation guidelines initially proposed by Guillemin et al.[24] and later revised by Beaton et al. [Figure 1].[25]

- Flowchart of the entire procedure of cross-cultural adaptation and validation of LEFS. LEFS: Lower extremity functional scale.
Stage 1 consisted of the initial translation of the LEFS into Sinhalese and its cross-cultural adaptation
Step 1: Translation
Initially, two highly qualified health professionals, both native Sinhalese speakers with extensive expertise in medical terminology, methodically and independently translated the LEFS into Sinhala (T1 and T2, respectively). Both are esteemed medical professors at the Faculty of Medicine, bringing a wealth of knowledge and experience to the translation process. One of them is the distinguished authorized author of the validated Sinhala version of the 12-Item General Health Questionnaire (GHQ-12), while the other is the respected authorized author of the validated Sinhala version of the World Health Organization QOFBref (WHOQOL-Bref). Their collective expertise ensured a precise and culturally appropriate translation of the LEFS. Afterward, there was a combined conversation to combine and integrate the two respective unique forms as a unified and harmonized version. During this phase, the investigators’ prime exertions were dedicated to accomplishing conceptual and linguistic similarity with the original English editions.
Step 2: Back translation
This meticulous process was carried out by two authorized and officially registered Sri Lankan government translators in strict accordance with the by-laws outlined in the Sri Lankan government constitution. These translators, with their deep understanding of both linguistic nuances and legal requirements, ensured that the translation adhered precisely to the highest standards of accuracy and cultural sensitivity. Their authoritative expertise, combined with their comprehensive knowledge of the official regulations, played a crucial role in producing a translation that is both legally compliant and linguistically faithful to the original text.
This process was performed entirely to ensure that the translated version of the questionnaire was grammatically sound and the terms incorporated were precise and accurate. Similarly, the essential meaning and detailed contents of the inventive LEFS were meticulously well preserved.
The two forward and backward translations were carefully reconciled, with a thorough sentence-by-sentence revision. The accuracy of the translations was evident, as both English back translations were remarkably similar to the original English version.
In a subsequent detailed discussion, the same authors precisely reviewed and incorporated the necessary changes, leading to the finalized translated questionnaire. On concluding this comprehensive procedure, we achieved a combined and refined version of the Sinhala LEFS.
Stage 2 – involved a prospective assessment of the Sinhalese version of LEFS’s critical psychometric properties using the finalized Sinhalese version (S-LEFS)
Step 01 – Selection of participants using inclusion and exclusion criteria
Step 02 – Enrolment and administration
Step 03 – Data collection and analysis.
Inclusion and exclusion criteria
Inclusion criteria
Proficiency in Sinhala: Participants were required to be fluent and highly proficient in the Sinhala language to ensure accurate understanding and communication
Age requirement: Participants had to be above 18 years old to be eligible for the study
Athletes with lower extremity disability: Athletes visiting the sports medicine clinic due to lower extremity disabilities were included to assess the functional impact of their conditions
Athletes undergoing pre-participation examination: Athletes attending the clinic for pre-participation examinations, who did not have any existing disabilities, were also included to provide a comparative baseline.
Exclusion criteria
Age below 18: Individuals under 18 years old were excluded from the study to ensure all participants were adults
Lower extremity fractures: Athletes with current fractures in the lower extremity were excluded due to the acute nature of their condition, which could interfere with the assessment of functional status.
Recent lower extremity surgeries: Athletes who had undergone recent lower extremity surgeries were excluded to avoid complications related to post-operative recovery that could affect their functional performance
Lack of written consent: Participants who did not provide written informed consent were excluded to ensure ethical compliance and agreement to participate in the study
Significant cognitive impairments: Individuals suffering from significant cognitive impairments, including all forms of dementia, severe traumatic brain injury, or profound mental retardation, were excluded to ensure accurate and reliable responses on the functional assessment.
Enrolment and administration
Considering that a key aim of this research was to systematically validate the Sinhala version of the LEFS (S-LEFS) through construct, convergent, and criterion validity, the respondents were carefully divided into two distinct groups. The case group consisted of athletes experiencing any lower extremity difficulties, while the control group comprised athletes without any lower limb dysfunction.
The cases and controls were matched by age, sex, and body mass index. The healthy athletes in the control group were mostly athletes who came to the sports and exercise medicine unit to do physical fitness tests, and the case group included athletes who came to take treatments for lower limb conditions. The sample size for factor analysis was determined by the number of items in the questionnaire, with a recommended minimum of five participants per item; hence, the final sample size was 146.[26,27] Eligible participants for this research were thoroughly advised on its intention and detailed procedure. After providing their written consent, each respondent was asked to complete a validated Sinhalese version of the WHOQOL-Bref[28] along with the Sinhalese version of the LEFS. The athletes were reassured of the strict privacy of the research.
Data collection and analysis
The translation and validation of the scale are detailed in Figure 1, with linguistic validity established as outlined in Mapi research trust guidelines. Face validity was determined by subject specialists who tested the questionnaire with an initial patient pool. Predictive validity, along with other forms of validity such as construct, convergent, and criterion validity, as well as sensitivity and specificity, were established through several independent studies. Internal consistency was measured using Cronbach’s alpha, while principal component analysis was employed to explore the underlying factors of the study and to understand how factor loadings related to meaningful themes, particularly in the newly developed questionnaire. During the clinical validation process, a validity and reliability test was conducted to confirm that the assessment tool accurately evaluates what it is intended to measure and consistently produces stable results across different conditions and over time.
Reliability
Reliability refers to the degree to which scores consistently persist equivalent with repetitive measurements when measured on the identical contributors.[29] To systematically assess the reliability, the internal consistency of the questionnaire was precisely estimated using Cronbach’s alpha coefficient. An alpha value of 0.7 or higher was deemed acceptable.
Construct validity
Construct validity represents the degree to which an instrument’s scores align and are consistent with the hypotheses, which are carefully expressed assuming that the tool accurately and genuinely evaluates the intended construct. The construct validity of the S-LEFS was evaluated by means of exploratory factor analysis (EFA), while its overall validity was assessed through a virtuous factor analysis among the 20 questions in the tool. Factor loadings of 0.4 or greater were believed to be satisfactory for this type of analysis.
Convergent validity
Convergent validity was carefully evaluated to illustrate the degree to which the LEFS correlates with another similar questionnaire. In this study, the WHOQOLBref was administered to evaluate convergent validity. WHOQOL-Bref assessed the QOF in 24 facets and QOF in general. Combining different facets, four domains have been developed to assess QOL. The main fields evaluated by WHOQOL-Bref were physical ability and capacity, psychological characteristics, social collaborations, living conditions, and environment. A distinct element was evaluated using a detailed five-point scale. A precise linear transformation was applied to standardize the raw scores. The scores ranged from 0 to 100, with higher values reflecting an elevated level of QOF. Pearson’s correlation coefficient (r) was utilized for this purpose, with an r = 0.4 or above being regarded as satisfactory and suggestive of a meaningful correlation.
Criterion validity
Further, as criterion validity, using the gold standard method, the consultant orthopedic surgeon’s decision (the gold standard) of having any lower limb condition was taken as positive for the disease when calculating specificity and sensitivity despite the degree of the disease. Each person was examined by an orthopedic surgeon who was blind to the LEFS scores of patients to analyze their lower limb condition. A receiver operating characteristic (ROC) curve was generated to compute the cutoff score of the LEFS for our local sample. The sensitivity of a test indicates the probability that the screening test might be positive among the diseased.[30] In contrast, the same screening test has the probability of being negative among those who have the disease. Exploring these two parameters is crucial when selecting a questionnaire to screen a target population. The adequacy of the sample size, comprising 112 athletes, was analyzed by applying Keiser– Meyer–Olkin and Hoteling’s T-squared values. All analytical tests were processed using the Statistical Package for the Social Sciences software 25.
RESULTS
The total number of participants was 146, and 34 of them refused to give written consent and did not fill out the questionnaires completely or satisfactorily. Consequently, a total of 112 questionnaires were carefully carried out once consent was granted. All 112 questionnaires were fully completed and then were incorporated into the subsequent evaluation and analyses. A total of 55 (49.11%) athletes were from the case group, and 57 (50.89%) athletes were from the control group. Athletes in the case group were identified as having lower extremity issues created by the hip, thigh, knee, leg, ankle, or foot. The Kaiser– Meyer–Olkin value found was 0.918, which was significant from a statistical standpoint (P < 0.0001). Equally, Bartlett’s Test of Sphericity had a significant value of P < 0.01. Accordingly, these detailed measurements clearly indicated the adequacy of the sample size used in this study.
Participants’ demographic data for each group is summarized in Table 1.
| Data category | Control group normal LL | Case group with LL abnormality | Total |
|---|---|---|---|
| Number of participants | 57 (50.89%) | 55 (49.11%) | 112 |
| Age (mean) | 37.95 years | 40.40 years | - |
| BMI | 24.37 | 24.96 | - |
| Gender | |||
| Male | 32 (56.14%) | 26 (47.27%) | 58 |
| Female | 25 (43.86%) | 29 (52.73%) | 54 |
| Married | 37 | 23 | 60 |
| Unmarried | 20 | 32 | 52 |
BMI: Body mass index, LL: Lower limb
Reliability
In this study, the value of Cronbach’s alpha was 0.952, demonstrating outstanding reliability, and similarly revealed the “Cronbach’s alpha value if the item was deleted,” which remains substantially greater value among the 20 questions (between 0.948 and 0.952). This finding significantly reinforces that the S-LEFS has strong internal consistency, indicating that all items contribute meaningfully to the scale and that none should be removed. This exceptional level of internal consistency suggests that the items are well-correlated and measure the same underlying construct, promising the S-LEFS a reliable tool for assessing lower extremity function.
Construct validity
The construct validity of the S-LEFS was evaluated through EFA. The unforced analysis, utilizing Varimax rotation, discovered the extraction of three distinct components [Table 2]. On further analysis, the recognized pattern allowed us to classify these three components according to the intensity of the activities. These three factors accounted for 70.63% of the cumulative variance [Table 3, Figure 2]. Component one referred to high-intensity activity, Component two referred to moderate-intensity activity, and Component three referred to low-intensity activity. As indicated in Table 2, entire items counted factor loadings >0.48, and all items displayed excellent outcomes. Similarly, entire items exhibited exceptionally high factor loadings, and each item was explicitly assigned to its appropriate particular domains. Item 06 exhibited the minimal factor loading value (0.46). Even though it had the smallest value, it was still deemed satisfactory. Item 20, “Rolling over in bed,” was expected to score a high factor loading in the low-intensity domain, yet it surprisingly registered a greater value in the moderate-intensity domain.
| Rotated component Matrixa | |||
|---|---|---|---|
| Component | |||
| 1 | 2 | 3 | |
| Q1. Any of your usual work, housework, or school activities | 0.767 | ||
| Q2. Your usual hobbies, recreational or sporting activities | 0.885 | ||
| Q3. Getting into or out of the bath. | 0.622 | 0.463 | |
| Q4. Walking between rooms. | 0.759 | ||
| Q5. Putting on your shoes or socks | 0.739 | ||
| Q6. Squatting | 0.460 | 0.429 | 0.400 |
| Q7. Lifting an object, like a bag of groceries, from the floor. | 0.432 | 0.717 | |
| Q8. Performing light activities around your home. | 0.561 | 0.467 | |
| Q9. Performing heavy activities around your home. | 0.493 | 0.499 | |
| Q10. Getting into or out of a car. | 0.786 | ||
| Q11. Walking 2 blocks | 0.466 | 0.721 | |
| Q12 Walking a mile. | 0.751 | 0.419 | |
| Q13. Going up or down 10 stairs (about 1 flight of stairs) | 0.597 | 0.631 | |
| Q14. Standing for 1 h. | 0.702 | ||
| Q15. Sitting for 1 h. | 0.554 | 0.474 | |
| Q16. Running on even ground. | 0.843 | ||
| Q17. Running on uneven ground. | 0.882 | ||
| Q18. Making sharp turns while running fast. | 0.859 | ||
| Q19. Hopping. | 0.841 | ||
| Q20. Rolling over in bed. | 0.462 | 0.403 | |
Extraction method: Principal component analysis. Rotation method: Varimax with Kaiser normalization. aRotation converged in 6 iterations
| Total variance explained | ||||||
|---|---|---|---|---|---|---|
| Component | Initial eigenvalues | Extraction sums of squared loadings | ||||
| Total | % of variance | Cumulative % | Total | % of variance | Cumulative % | |
| 1 | 10.745 | 53.727 | 53.727 | 10.745 | 53.727 | 53.727 |
| 2 | 2.056 | 10.282 | 64.009 | 2.056 | 10.282 | 64.009 |
| 3 | 1.326 | 6.629 | 70.638 | 1.326 | 6.629 | 70.638 |
| 4 | 0.900 | 4.500 | 75.138 | |||
| 5 | 0.699 | 3.493 | 78.631 | |||
| 6 | 0.549 | 2.747 | 81.379 | |||
| 7 | 0.523 | 2.615 | 83.993 | |||
| 8 | 0.482 | 2.409 | 86.402 | |||
| 9 | 0.436 | 2.181 | 88.584 | |||
| 10 | 0.358 | 1.791 | 90.375 | |||
| 11 | 0.307 | 1.537 | 91.912 | |||
| 12 | 0.297 | 1.485 | 93.397 | |||
| 13 | 0.237 | 1.187 | 94.584 | |||
| 14 | 0.210 | 1.050 | 95.634 | |||
| 15 | 0.185 | 0.926 | 96.560 | |||
| 16 | 0.166 | 0.832 | 97.393 | |||
| 17 | 0.156 | 0.781 | 98.174 | |||
| 18 | 0.143 | 0.717 | 98.891 | |||
| 19 | 0.126 | 0.629 | 99.520 | |||
| 20 | 0.096 | 0.480 | 100.000 | |||
Extraction method: Principal component analysis: The only Eigenvalue above 1.0 is mentioned. LEFS: Lower extremity functional scale
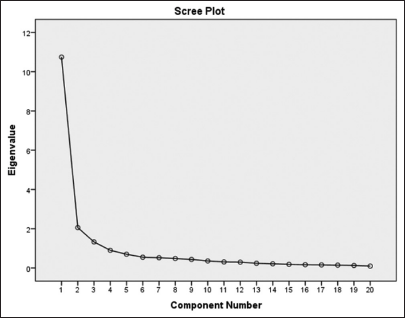
- The scree plot of the principal component analysis.
Convergent validity
Convergent validity was determined from the correlation between S-LEFS and WHOQOL-Bref. However, the overall score between S-LEFS and WHOQOL-Bref was very poorly correlated, having r = 0.281. The correlation among S-LEFS and components of WHOQOL-Bref also demonstrated a poor value of “r” consisting of physical (r = 0.396), psychological (r = 0.169), social (r = 0.202), and environmental (r = 0.094).
Criterion validity
With reference to criterion validity, an ROC curve was generated to compute the cutoff score of the LEFS. In this study, the scale was analyzed against clinical judgment as the gold standard. Athletes who did not have any lower extremity dysfunction or injury were considered normal participants in the study. Individuals who counted high total LEFS scores were thought to have optimal lower extremity function. With regard to this study, to clarify the sensitivity and specificity metrics, the following detailed analysis was performed. The area under the ROC curve for the LEFS was 0.938, indicating an exceptional ability of the scale to differentiate between athletes with and without lower extremity abnormalities. The ROC curve’s area under the curve (AUC) ranges from 0.5, representing no discrimination, to 1.0, representing perfect discrimination, with a value above 0.9 demonstrating outstanding performance. The study established a cutoff point of 67.5 for the LEFS score, chosen to balance sensitivity and specificity effectively. At this threshold, the LEFS exhibited a sensitivity of 87.5%, meaning it correctly identified 87.5% of athletes with lower extremity abnormalities as having a problem, thus showcasing high precision in detecting affected individuals. In addition, the scale achieved a specificity of 83%, indicating that 83% of athletes without lower extremity abnormalities were correctly classified as not having a problem, demonstrating its robust capacity to accurately classify those without the condition. Overall, these metrics were derived from comparing LEFS scores against a known diagnostic standard, with the high sensitivity reflecting the scale’s effectiveness in identifying abnormalities and the good specificity showing its ability to correctly identify non-affected athletes. The AUC of 0.938 further underscores the LEFS’s excellent performance in distinguishing between affected and non-affected athletes [Figure 3].
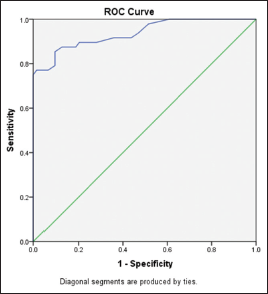
- Receiver operating characteristic (ROC) curve.
DISCUSSION
It should be emphasized that, when assessing the health-related QOF, particularly in relation to the lower extremities, there is a prerequisite for an instrument to measure. Hence, this study is conducted to overcome this problem. As a self-report questionnaire, [Figure 4] LEFS offers us vital pertinency in both educational and clinical backgrounds. Hence, it is crucial to consistently employ a thoroughly validated and reliable health-related outcome measure. To be more specific, both culturally and linguistically appropriate adaptation might be obligatory to ensure it is a validated instrument. During the initial development of the LEFS, statistical analysis was applied to assess its reliability and validity. The findings were then compared to the SF-36 scores to determine the scale’s effectiveness. In this study, excellent results were obtained, though the methodology was different, with exceptionally high factor loading still achieved for all 20 items. To put it differently, it should be elaborated that entirely 20 questions included in the LEFS questionnaire are highly valid and reliably formulated questions to comprehensively assess various aspects of lower extremity function. The inventive author of the LEFS did not express it; however, this study managed to extract effectively three domains across the entire 20-item questionnaire. One of the domains appeared to comprise high-intensity activity (Questions 6, 12, 14, 15, 16, 17, 18, and 19), and the second seemed to involve moderate-intensity activity (Questions 3, 4, 5, 8, 10, 11, 13, and 20). Questions 1, 2, 7, and 9 were categorized as low-intensity activities; nevertheless, all scored a prominent factor loading of more than 0.4. The Cronbach’s alpha values in the original study of the LEFS development were remarkably high, measuring 0.96, and similarly, 0.952 in this study, both of which are outstanding. This emphasized the LEFS questionnaire’s exceptional ability to effectively distinguish between lower extremities with normal function and those experiencing issues, as demonstrated in both the original Binkley study and this research. Precisely speaking, one of the significant strengths of this present study was the exceptionally high measure of internal consistency, with a Cronbach’s alpha value of r = 0.952. This value is remarkably similar in comparison to other numerous cross-cultural adaptation studies that have translated the English version of the LEFS into various languages. Notably, in the Dutch version, the overall Cronbach’s alpha value for all 20 objects was an impressive 0.96. Similarly, an additional remarkable strong point of this research was its sufficiently large quantity of the sample, as evidenced by the statistically significant results of the Kaiser–Meyer–Olkin measure and Bartlett’s Test of Sphericity. These tests demonstrated a highly significant value, thereby demonstrating a substantial and reliable power of analysis.
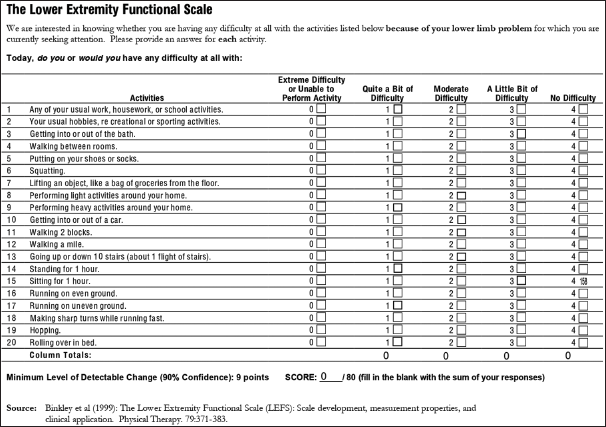
- Lower extremity functional scale original version English.
In this present study, based on expert opinions, several key changes were thoughtfully implemented to ensure that the LEFS was culturally adapted across the entirety of Sri Lanka. Specifically, in adapting the LEFS from its English version to Sinhala, questions 3, 5, 10, 11, and 20 were slightly modified to better fit the context of the Sri Lankan population, ensuring the scale remains relevant and appropriate for local use.
Bathing: The English version of Question 3 asks about “Getting into or out of the bath,” which was revised in the Sinhala version to simply “Bathing.” This change was necessary because bathtubs are not commonly used in Sri Lanka; most people bathe using showers or other methods.
Footwear: Question 5 in the English version is “Putting on your shoes or socks.” In the Sinhala version, this was expanded to “Putting on your shoes, socks, or slippers” to reflect the common practice in Sri Lanka of wearing slippers in addition to or instead of shoes and socks.
Transportation: The English version’s Question 10, “Getting into or out of a car,” was modified to “Getting into or out of a vehicle” in the Sinhala version. This adjustment acknowledges the widespread use of public transport and the variability in vehicle types used in Sri Lanka.
Walking Distance: Question 12 in the English version refers to “Walking for 2 blocks.” This was adapted to “Walking for 150 m (500 steps)” in the Sinhala version because the concept of city blocks is not commonly used in Sri Lanka; instead, distances are typically measured in meters.
Sleeping Surface: The English version’s Question 20, “Rolling over in bed,” was changed to “Rolling over in bed or on a mat” in the Sinhala version. This change accommodates the practice of sleeping on mats on the floor, which is common in many Sri Lankan households.
These modifications ensure that the Sinhala version of the LEFS [Figure 5] accurately reflects the daily life and cultural practices of the Sri Lankan population, improving the scale’s relevance and utility in assessing lower extremity function within this specific context.
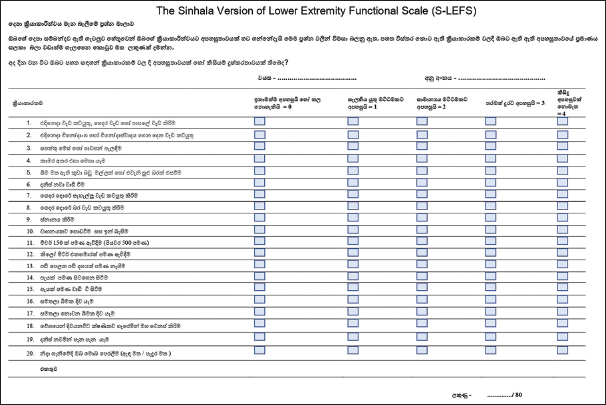
- Lower extremity functional scale Sinhala version (Cross culturally adapted and validated).
In addition, Question 9 (Performing heavy activities around your home) should be categorized under component two (moderate-intensity activity) instead of component three. Similarly, Question 20 (rolling over in bed) should be classified under component three (low-intensity activity) instead of component two. It should be emphasized that these minor changes to the original version of the LEFS have been cross-culturally adapted into the Sinhala version of the LEFS, and it remains statistically highly reliable.
Furthermore, this study was precisely expanded to thoroughly test the psychometric properties of the S-LEFS, in contrast to the Sinhala language version of the WHOQOL-Bref, as many scholars regard this standardized comparison as essential. However, the correlation of the total score between S-LEFS and WHOQOL-Bref was insignificant since the WHOQOLBref has not been adequately questioned about the lower limb disability. Similarly, its other components, such as psychological, social, and environmental, were also not correlated significantly.
The S-LEFS offers several key benefits and applications in sports medicine in Sri Lanka. Initially, it provides a comprehensive baseline measurement of an athlete’s lower extremity function, establishing a clear understanding of the injury’s or condition’s impact on daily activities and sports performance. Regular administration of the S-LEFS allows for systematic tracking of recovery over time, enabling clinicians to objectively document improvements or setbacks and adjust treatment plans as needed. The detailed data from the S-LEFS facilitate the setting of realistic, specific rehabilitation goals tailored to individual needs, guiding the development of personalized rehabilitation programs. This tailored approach helps address specific functional deficits, prioritize interventions, and optimize the rehabilitation process for better athletic performance and outcomes. In addition, the S-LEFS is instrumental in evaluating the overall success of treatment interventions by comparing final outcomes with initial baselines, aiding in decisions about the athlete’s readiness to return to sport. It also enhances communication between athletes and health-care providers by providing clear, objective data on functional progress, helping athletes understand their recovery trajectory and stay engaged in their rehabilitation. Validating the S-LEFS for broader use across different regions and populations in Sri Lanka can significantly enhance its value in sports medicine. It will not only improve the consistency and quality of care provided to athletes but also contribute to a more standardized approach to assessing and managing lower extremity conditions. In summary, the S-LEFS is a powerful tool for sports medicine practitioners in Sri Lanka. Its use in routine assessments can help in setting precise treatment goals, monitoring progress, and tailoring rehabilitation programs, ultimately leading to more effective and personalized care for athletes with lower extremity conditions.
Study strengths and limitations
The strengths of the research comprise the prospective nature and the acceptable quantity of participants that provided an appropriate sample size and power of analysis. The insertion of a consecutive series of athletes, along with the impartiality of the evaluators and diverse recommendation sources, along with the wide range of diagnoses and group representations, strongly recommends minimal selection bias and enhances the potential for universal applicability.
However, a key limitation of this study is that its findings are applicable only to the Sinhala-speaking population in Sri Lanka. To extend the applicability of the results, future research should include participants from Tamil, Muslim, and Burgher ethnic groups. This would help ascertain whether linguistic and cultural differences influence the LEFS’s effectiveness and accuracy, considering the diverse ethnic backgrounds within Sri Lanka. In addition, the study focused exclusively on athletes with lower extremity conditions. However, the LEFS was originally designed to assess a wide range of lower extremity issues across various patient populations. Including a broader spectrum of patients with different lower extremity conditions in future research would provide a more comprehensive evaluation of the tool’s utility and effectiveness. Expanding research to include other languages and cultural groups will enhance the LEFS’s overall applicability and ensure its relevance across diverse populations.
CONCLUSION
For the very first time, the original version of LEFS was successfully and precisely cross-culturally adapted into the Sinhala language. The psychometric properties of the S-LEFS have been reported to be exceptionally strong, especially with regard to internal consistency, reliability, and validity. This comprehensive adaptation makes the S-LEFS a highly reliable and valid tool for assessing lower limb function in Sinhala-speaking athletes who are experiencing musculoskeletal dysfunction in the lower extremities. Given its thorough validation, the S-LEFS can be confidently employed in both clinical and research settings to accurately evaluate and monitor lower limb functionality among this specific population.
Acknowledgments
I would also like to acknowledge the dedicated efforts of the Professors, Doctors, physiotherapists, masseurs, and medical staff of the Sports Medicine Unit whose collaboration and support were integral to the success of this study. Last but not least, my heartfelt appreciation goes to all the athletes whose contribution and commitment made this study possible.
Author contributions
STT: Concept and design, data acquisition and analysis, drafting, revision, and final approval.
Ethical approval
The research/study approved by the Institutional Review Board at Faculty of Medicine University of Ruhuna, number 2021.P.001 (12/01/2021), dated March 17, 2021.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The author confirms that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Measurement properties of the German version of the IKDC subjective knee form (IKDC-SKF) J Patient Rep Outcomes. 2018;2:31.
- [CrossRef] [PubMed] [Google Scholar]
- Cross-cultural adaptation and measurement properties of the Brazilian Portuguese version of the Victorian institute of sport assessment-Achilles (VISA-A) questionnaire. J Orthop Sports Phys Ther. 2018;48:567-73.
- [CrossRef] [PubMed] [Google Scholar]
- Structural and physical-functional deficits in lower limbs with fractures and treated surgically. Fisioter Mov. 2018;31:e003138.
- [CrossRef] [Google Scholar]
- Reliability and validity of the hip stability isometric test (HipSIT): A new method to assess hip posterolateral muscle strength. J Orthop Sports Phys Ther. 2017;47:906-13.
- [CrossRef] [PubMed] [Google Scholar]
- Validation study of WOMAC: A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol. 1988;15:1833-40.
- [Google Scholar]
- Hip disability and osteoarthritis outcome score (HOOS)--validity and responsiveness in total hip replacement. BMC Musculoskelet Disord. 2003;4:10.
- [CrossRef] [PubMed] [Google Scholar]
- EQ-5D and the EuroQol group: Past, present and future. Appl Health Econ Health Policy. 2017;15:127-37.
- [CrossRef] [PubMed] [Google Scholar]
- The MOS 36-item short-form health survey (SF-36) I. Conceptual framework and item selection. Med Care. 1992;30:473-83.
- [CrossRef] [PubMed] [Google Scholar]
- Determinants of pain, disability, health-related quality of life and physical performance in patients with knee osteoarthritis awaiting total joint arthroplasty. Disabil Rehabil. 2018;40:2734-44.
- [CrossRef] [PubMed] [Google Scholar]
- Does the addition of hip strengthening exercises improve outcomes following total knee arthroplasty? A study protocol for a randomized trial. BMC Musculoskelet Disord. 2016;17:259.
- [CrossRef] [PubMed] [Google Scholar]
- The lower extremity functional scale (LEFS): Scale development, measurement properties, and clinical application. Phys Ther. 1999;79:371-83.
- [CrossRef] [Google Scholar]
- The German Lower Extremity Functional Scale (LEFS) is reliable, valid and responsive in patients undergoing hip or knee replacement. Qual Life Res. 2015;24:405-10.
- [CrossRef] [PubMed] [Google Scholar]
- Cross-cultural adaptation and validation of the simplified Chinese version of the lower extremity functional scale. Biomed Res Int. 2020;2020:1421429.
- [CrossRef] [PubMed] [Google Scholar]
- Reliability and validity of the Turkish version of the lower extremity functional scale in patients with different lower limb musculoskeletal dysfunctions. Int J Ther Rehabil. 2019;26
- [CrossRef] [Google Scholar]
- Cross-cultural adaptation, validity and reliability of the Arabic version of the Lower Extremity Functional Scale. Disabil Rehabil. 2016;38:897-904.
- [CrossRef] [PubMed] [Google Scholar]
- Association of pain catastrophizing with static balance, mobility, or functional capacity in patients with knee osteoarthritis: A blind cross-sectional study. J Manipulative Physiol Ther. 2018;41:42-6.
- [CrossRef] [PubMed] [Google Scholar]
- Understanding posterior meniscal roots lesions: From basic science to treatment. Rev Bras Ortop. 2017;52:463-72.
- [CrossRef] [PubMed] [Google Scholar]
- The Italian version of the lower extremity functional scale was reliable, valid, and responsive. J Clin Epidemiol. 2010;63:550-7.
- [CrossRef] [PubMed] [Google Scholar]
- The Dutch Lower Extremity Functional Scale was highly reliable, valid and responsive in individuals with hip/knee osteoarthritis: A validation study. BMC Musculoskelet Disord. 2012;13:117.
- [CrossRef] [PubMed] [Google Scholar]
- Reliability and validity of the Persian lower extremity functional scale (LEFS) in a heterogeneous sample of outpatients with lower limb musculoskeletal disorders. Disabil Rehabil. 2014;36:10-5.
- [CrossRef] [PubMed] [Google Scholar]
- Translation, cross-cultural adaptation and analysis of the psychometric properties of the lower extremity functional scale (LEFS): LEFS-Brazil. Brazilian J Phys Ther. 2013;17:272-80.
- [CrossRef] [PubMed] [Google Scholar]
- Lower Extremity Functional scale (LEFS): Cross-cultural adaption into Greek and reliability properties of the instrument. Health Sci J. 2012;6:750-73.
- [Google Scholar]
- Construct and criterion validity of the Malaysia version of Lower Extremity Functional Scale (LEFS) Asia Pac J Sport Med Arthrosc Rehabil Technol. 2017;10:8-11.
- [CrossRef] [PubMed] [Google Scholar]
- Cross-cultural adaptation of HRQL measures: Literature review and proposed guidelines. J Clin Epidemiol. 1993;46:1417-32.
- [CrossRef] [PubMed] [Google Scholar]
- The DASH (disabilities of the arm, shoulder and hand) outcome measure: What do we know about it now? Br J Hand Ther. 2001;6:109-18.
- [CrossRef] [Google Scholar]
- Optimal sample size determination for the ANOVA designs. Int J Appl Math Stat. 2012;25:127-34.
- [Google Scholar]
- The research question in clinical practice: A guideline for its formulation. Rev Colomb Psiquiatr. 2018;47:193-200.
- [CrossRef] [PubMed] [Google Scholar]
- Assessment of quality of life using Sinhala translation of WHO QOL-100. Galle Med J. 2003;4:46.
- [Google Scholar]
- Knee synergism during gait remain altered one year after ACL reconstruction. Acta Ortop Bras. 2016;24:137-41.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical tests: Sensitivity and specificity. Contin Educ Anaesth Crit Care Pain. 2008;8:221-3.
- [CrossRef] [Google Scholar]




