
Translate this page into:
Injury profile in badminton players of Asian countries: A systematic review and meta-analysis

*Corresponding author: Pulak Sharma, Department of Orthopaedics, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow, Uttar Pradesh, India. drpulaksharma@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Sharma P, Samant N, Keshav K, Mishra S. Injury profile in badminton players of Asian countries: A systematic review and meta-analysis. J Arthrosc Surg Sports Med. doi: 10.25259/JASSM_51_2024
Abstract
Background and Aims
Badminton is a globally acknowledged non-contact racquet sport that requires agility, strategic insight, and precise execution. It is important to note that a considerable number of elite badminton players across different formats originate from Asia. Consequently, it is essential to analyze the epidemiological patterns of injuries to formulate effective injury prevention strategies. The review aimed to study the epidemiological pattern of badminton injuries and describe injury contexts and characteristics in countries of the Asian Region.
Materials and Methods
PubMed, Scopus, and Embase were searched using words related to badminton and injury. Badminton players of Asian countries from the recreational to international levels who play in all formats of the game were included in the study. There was no restriction on the age of the badminton players. Methodological quality was independently evaluated by two authors using the Joanna Briggs Institute (JBI) critical appraisal instruments.
Results
Following a thorough screening based on established inclusion and exclusion criteria, eight studies were incorporated into the review. These studies provided data concerning 1265 badminton players ranging from adolescents to adults. In total, 2284 injuries were examined. The aggregated data indicated that the majority of these injuries affected the lower limbs and were predominantly classified as overuse injuries.
Conclusion
The injury data presented in this review serves as a valuable resource for the development of injury-prevention programs, aimed at mitigating the incidence of injuries and thereby enhancing player availability. A significant concern highlighted in the review is the need for standardization in injury reporting formats and documentation, which is essential for achieving these objectives effectively.
Keywords
Asia
Badminton
Epidemiology
Injuries
Meta-analysis
Systematic review

INTRODUCTION
Badminton is a highly regarded non-contact racquet sport that requires agility, strategic insight, and precise execution. The sport’s widespread appeal can be attributed to its inclusive nature; it is enjoyed recreationally by individuals of varying skill levels and is often regarded as a family-friendly activity. Moreover, the competitive landscape has flourished with numerous tournaments held at both national and international levels. These events not only highlight elite athletes but also serve to inspire younger generations to participate in the sport. As a result, these factors have played a pivotal role in significantly enhancing the popularity of badminton across diverse regions globally, with a pronounced impact observed particularly in Asia.[1]
Although badminton is categorized as a non-contact sport with comparatively lower injury rates than contact sports, it involves high-speed movements and varied body postures that place considerable physical demands on participants.[2] Although the nature of the game reduces direct physical confrontation between players, participants remain vulnerable to various forms of overuse and traumatic injuries. This concern is pertinent to players across all age groups.[3]
According to the Badminton World Federation, approximately 150 million individuals participate in badminton globally. Furthermore, around 2000 players engage in international competitions.[4] The physically demanding nature of the game, coupled with brief resting periods, significantly increases the risk of injuries to both upper and lower extremities. A comprehensive analysis of these badminton-related injuries will provide valuable insights for coaches and athletes, thereby aiding in the reduction of injury risks among badminton players.[5]
It is noteworthy that a significant number of elite badminton players across various formats of the game originate from Asia. However, to date, there has been no comprehensive review examining the epidemiological nature of badminton-related injuries within this region. As a result, this systematic review aims to analyze the existing literature on badminton injuries in Asia with the objective of elucidating epidemiological injury patterns and contributing to the development of effective injury prevention strategies.
MATERIALS AND METHODS
Protocol and registration
The systematic review was registered in PROSPERO (CRD42024543738) and reported in accordance with the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines.
Review question
The primary aim is to review the epidemiology of sports-related injuries in badminton players. The secondary aim is to describe injury contexts and characteristics (i.e., location, nature, incidence proportion, and clinical incidence) of injuries in badminton players.
Selection criteria
Participants
Badminton players from recreational to international level. There was no restriction on the age or sex of the players.
Condition
Sports-related injuries involved in badminton players excluding illness or other health problems. There was no restriction on the definition of the term “injury” but studies using the same definition will be grouped for better analyses and comparisons.
Types of studies
Inclusion criteria
Original research such as observational studies, prospective or retrospective, cohort studies, and cross-sectional surveys.
Exclusion criteria
Studies involving multiple sports
Studies which are published in other languages except English
Studies that recruited participants with a specific pathology
Multiple publications for studies involving the same cohort
Studies published after 2000
Studies outside the Asian region.
Search strategy
Online databases of PubMed, Scopus, and Embase related to badminton and injury.
Study selection and screening
All identified searches were systematically collated using EndNote 21, with duplicates subsequently removed. The titles and abstracts underwent independent screening by two authors in accordance with the predefined inclusion and exclusion criteria. Full-text articles of the shortlisted studies were then obtained and independently reviewed by the same two authors, leading to the exclusion of studies that did not meet the inclusion criteria. Any disagreements concerning study inclusion or exclusion were resolved through discussion between the two reviewers, with a third reviewer serving as an adjudicator when necessary.
Assessment of methodological quality
Methodological quality was independently evaluated by two authors using the Joanna Briggs Institute (JBI) critical appraisal instruments. The JBI critical appraisal checklist for prevalence studies provided a numerical score out of a possible 9 points [Table 1]. The JBI critical appraisal checklist for cohort studies provided a numerical score out of a possible 11 points [Table 2]. Studies characterized by low-to-moderate risk of bias were incorporated into the data synthesis. Any discrepancies in methodological quality scoring were resolved through consultation with a third author.
| Item | Gasibat et al. | Shariff et al. | Karyono et al. | Total % |
|---|---|---|---|---|
| 1. Was the sample frame appropriate to address the target population? | Y | Y | Y | 100 |
| 2. Were study participants sampled in an appropriate way? | Y | Y | Y | 100 |
| 3. Was the sample size adequate? | Y | Y | Y | 100 |
| 4. Were the study subjects and the setting described in detail? | Y | Y | Y | 100 |
| 5. Was the data analysis conducted with sufficient coverage of the identified sample? | Y | Y | Y | 100 |
| 6. Were valid methods used for the identification of the condition? | Y | Y | N | 66.66 |
| 7. Was the condition measured in a standard, reliable way for all participants? | Y | Y | N | 66.66 |
| 8. Was there appropriate statistical analysis? | Y | Y | Y | 100 |
| 9. Was the response rate adequate, and if not, was the low response rate managed appropriately? | Y | Y | Y | 100 |
| Score | 9/9 | 9/9 | 8/9 | |
| Risk of bias | Low | Low | Low |
JBI: Joanna Briggs Institute
| Item | Goh et al. | Rangasamy et al. | Suryanto et al. | Zhou et al. | Miyake et al. | Total % |
|---|---|---|---|---|---|---|
| 1. Were the two groups similar and recruited from the same population? | Y | Y | Y | Y | Y | 100 |
| 2. Were the exposures measured similarly to assign people to both exposed and unexposed groups? | Y | Y | Y | Y | Y | 100 |
| 3. Was the exposure measured in a valid and reliable way? | Y | Y | Y | Y | Y | 100 |
| 4. Were confounding factors identified? | Y | Y | Y | Y | Y | 100 |
| 5. Were strategies to deal with confounding factors stated? | Y | Y | Y | Y | Y | 100 |
| 6. Were the groups/participants free of the outcome at the start of the study (or at the moment of exposure)? | Y | Y | Y | Y | Y | 100 |
| 7. Were the outcomes measured in a valid and reliable way? | Y | Y | Y | Y | Y | 100 |
| 8. Was the follow up time reported and sufficient to be long enough for outcomes to occur? | Y | Y | Y | Y | Y | 100 |
| 9. Was follow up complete, and if not, were the reasons to loss to follow up described and explored? | Y | Y | Y | Y | Y | 100 |
| 10. Were strategies to address incomplete follow up utilized? | N/A | N/A | N/A | N/A | N/A | 0 |
| 11. Was appropriate statistical analysis used? | Y | Y | Y | Y | Y | 100 |
| Score | 10/10 | 10/10 | 10/10 | 10/10 | 10/10 | 100 |
| Risk of bias | Low | Low | Low | Low | Low |
JBI: Joanna Briggs Institute
Data extraction
The extracted information regarding participants and study characteristics encompassed the type of study, country of origin, and injury data. The injury data comprised details on the definition of injury, nature of injuries, overuse injuries, incidence proportion, clinical incidence, likelihood of injuries occurring, training or playing hours per week, and the anatomical regions affected.[2]
Formulas:
Odds of Injuries= Number of injured players/Number of injury-free players
Incidence Proportion = Number of injured athletes/Number of athletes at risk
Clinical Incidence = Number of injuries/Number of athletes at risk.
Data synthesis
For data synthesis, we first provided a description of the methods and the population of the included studies. Then, we described the primary and secondary outcomes for each study and tried to combine the information to propose a summary of the outcomes according to subgroups (described below):
Anatomical region affected by injury
Nature of injury
Overuse injury
Incidence proportion.
Statistical analysis
A random-effect model was employed to account for heterogeneity and to adjust the pooled estimate of effects across the included studies. To evaluate heterogeneity among studies, both the Chi-square test and Tau2 test were utilized, whereas the I2 statistic was used to quantify the overall variability, expressed as a percentage. According to Higgins and Thompson, I2 values are categorized into low, moderate, and high levels of heterogeneity. Funnel plots were created to visualize heterogeneity and evaluate potential publication bias by fail-safe N analysis, which was computed using the Rosenthal approach. In addition, forest plots were generated to estimate the point estimates (proportions) along with their 95% confidence intervals (95% CI). In these forest plots, the lines on either side of each estimate represent the 95% CI, and the size of the squares indicates the weight of each study. The meta-analysis was performed using Jamovi 2.3.28 software.
RESULTS
Study inclusion
All three databases, namely PubMed, Scopus, and Embase were searched on April 3, 2024. A total of 2859 records were obtained from the search. The latest version of Endnote, i.e., Endnote 21 was used for collation of studies and to identify and remove duplicates. 808 records were identified as duplicates and removed. Out of the remaining 2051 records, 1929 records were excluded based on a review of the title. The remaining 122 records were subjected to a more detailed evaluation and further, 104 records were excluded on the basis of title and abstract. These 18 reports were sought for retrieval, but 4 reports were not retrievable. Hence, 14 reports were assessed for eligibility based on the inclusion and exclusion criteria. Out of these 14 reports, 6 were excluded and 8 reports were included in the review (PRISMA Diag.) [Figure 1].
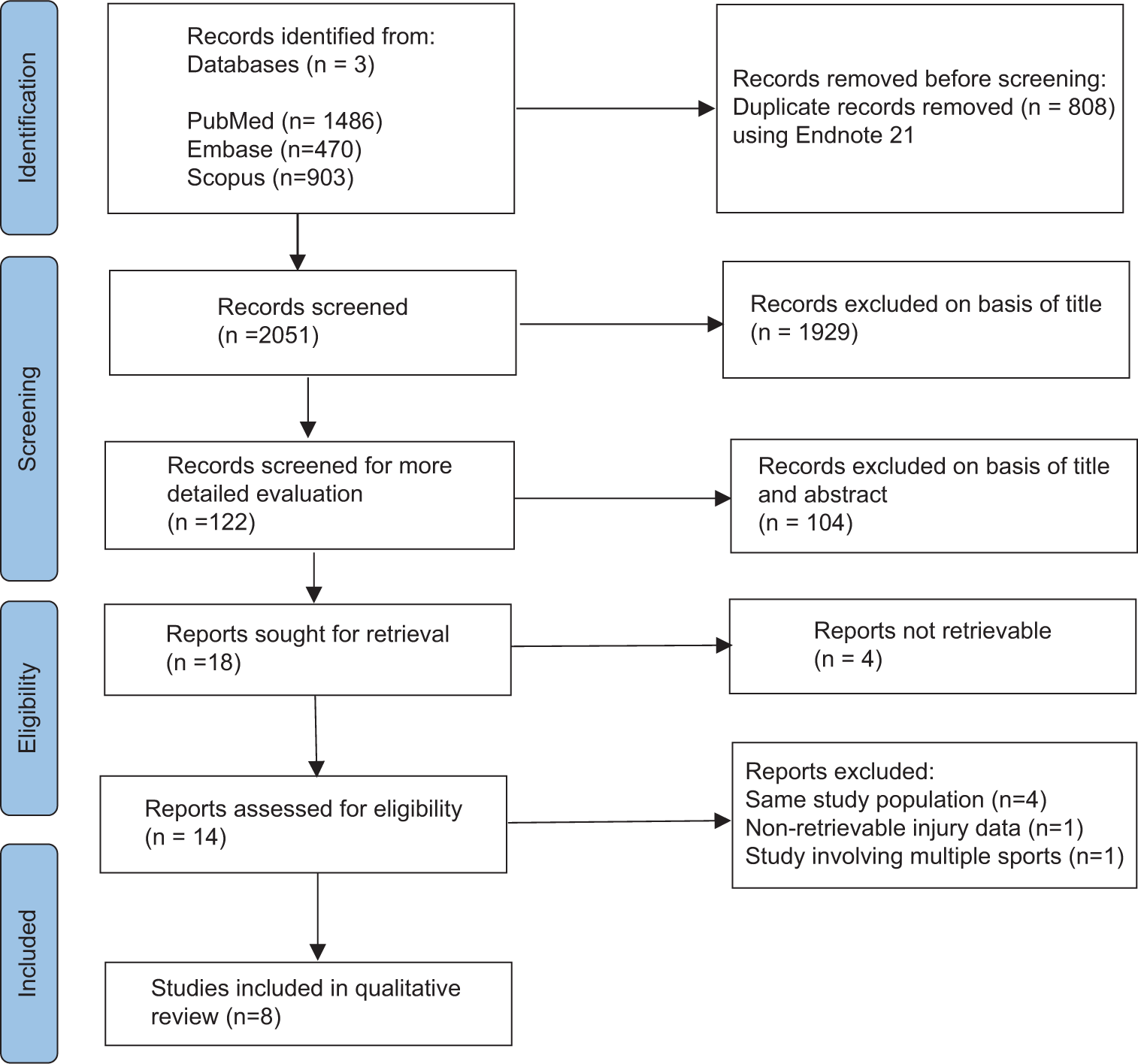
- Preferred reporting items for systematic reviews and meta-analyses flow diagram.
Characteristics of included studies
A total of 2284 injuries were reviewed and data from 1265 badminton players from adolescent to adult were extracted from the eight studies.
Among the reviewed studies, three were prevalence studies[3,5,6] and five were cohort studies.[1,2,7-9]
Three studies[2,3,6] were from Malaysia, two studies[1,5] were from Indonesia, two[8,9] were from Japan, and one study[7] was from India [Figure 2].
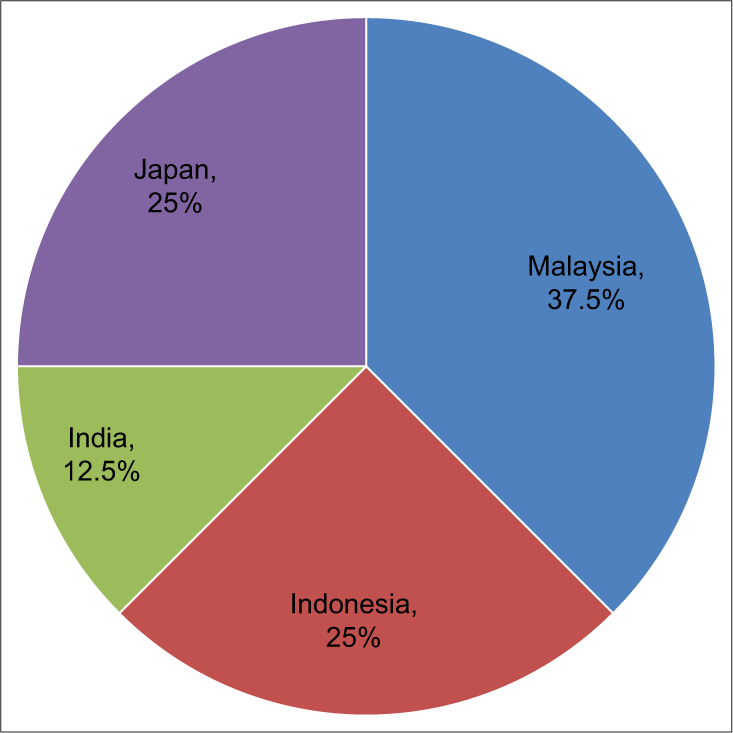
- Country-wise distribution of studies reviewed.
In accordance with the JBI critical appraisal checklist for assessing methodological quality in prevalence studies, a numerical score exceeding 6 is deemed to indicate a low risk of bias. Scores ranging from 4 to 6 are categorized as representing a moderate risk of bias, whereas scores below 4 are designated as indicating a high risk of bias. This evaluation is based on a total possible numerical score of 9. Subsequent to the analysis, it was determined that among the three prevalence studies examined, all three studies demonstrated a low risk of bias. Hence, all three studies were subsequently incorporated into the data synthesis process [Table 1].
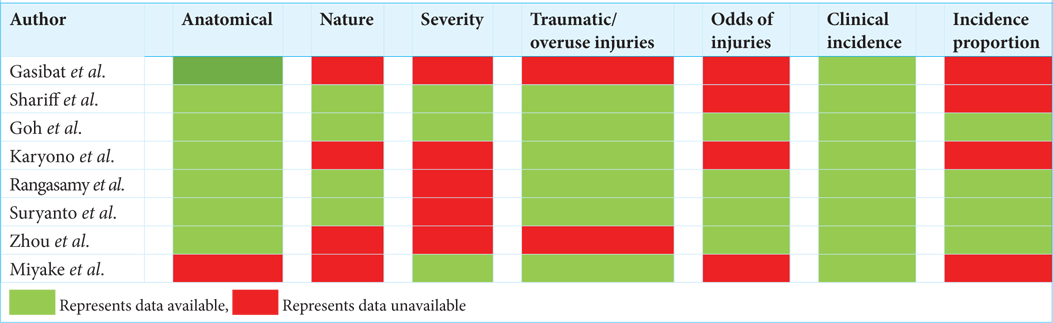
When dealing with cohort studies according to the JBI critical appraisal checklist, a numerical score exceeding 7 was classified as low risk of bias, whereas scores ranging from 4 to 7 were categorized as moderate risk of bias. Scores below 4 were designated as high risk of bias. The data synthesis incorporated all five cohort studies as they were determined to have a low risk of bias [Table 2]. Distribution of data extracted from the screened studies are represented below [Table 3]. Various other data such as odds of injuries, clinical incidence and incidence proportion [Table 4] and the percentage of traumatic and overuse injuries [Table 5] were also extracted from the studies included.
 |
| Author | Odds of injuries | Clinical incidence | Incidence proportion |
|---|---|---|---|
| Gasibat et al. | 3.15 | ||
| Shariff et al. | 2.47 | ||
| Goh et al. | 1.32 | 1.09 | 0.57 |
| Karyono et al. | 5.29 | ||
| Rangasamy et al. | 1.37 | 1.06 | 0.58 |
| Suryanto et al. | 0.22 | 0.19 | 0.18 |
| Zhou et al. | 1.56 | 1.51 | 0.61 |
| Miyake et al. | 2.03 |
| Author | Traumatic injuries (players) (%) | Overuse injuries (players) (%) |
|---|---|---|
| Shariff et al. | 300 (63.9) | 169 (36) |
| Goh et al. | 46 (73) | 16 (25.4) |
| Karyono et al. | 39 (48.75) | 41 (51.25) |
| Rangasamy et al. | 204 (81.27) | 47 (18.72) |
| Suryanto et al. | 13 (54.2) | 11 (45.8) |
| Miyake et al. | 70 (25.92) | 200 (74.1) |
Incidence proportion of injuries
The random-effects model, drawn from 4 studies, revealed a pooled data of 48.3% for the incidence proportion of injuries (95% CI: 28.1–68.5; P < 0.001). The pooled estimate of effects in this meta-analysis showed substantial heterogeneity among studies (I2 = 97.11%, P < 0.001). The funnel plot, when visually inspected, suggested an asymmetry and demonstrated publication bias (Fail-safe n = 1154, P < 0.001) [Figure 3].
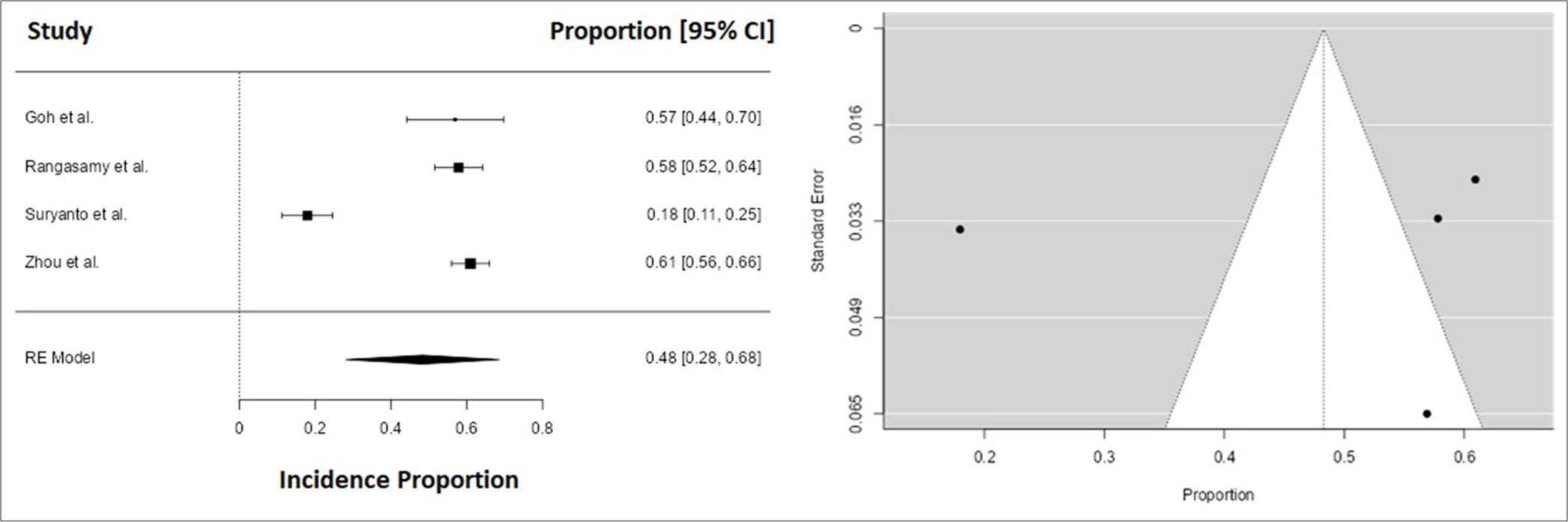
- Forest and funnel plot depicting incidence proportion.
Distribution of injuries sustained by body region
Three studies reported a majority of upper extremity injuries, of which one study reported the maximum percentage, i.e., 45.42%.[7] One study reported back injury to be the most common, i.e., 30.87%,[3] whereas, two studies reported a majority of lower extremity injuries with 71.43%[2] and 74%,[5] respectively [Figure 4 and Table 6].
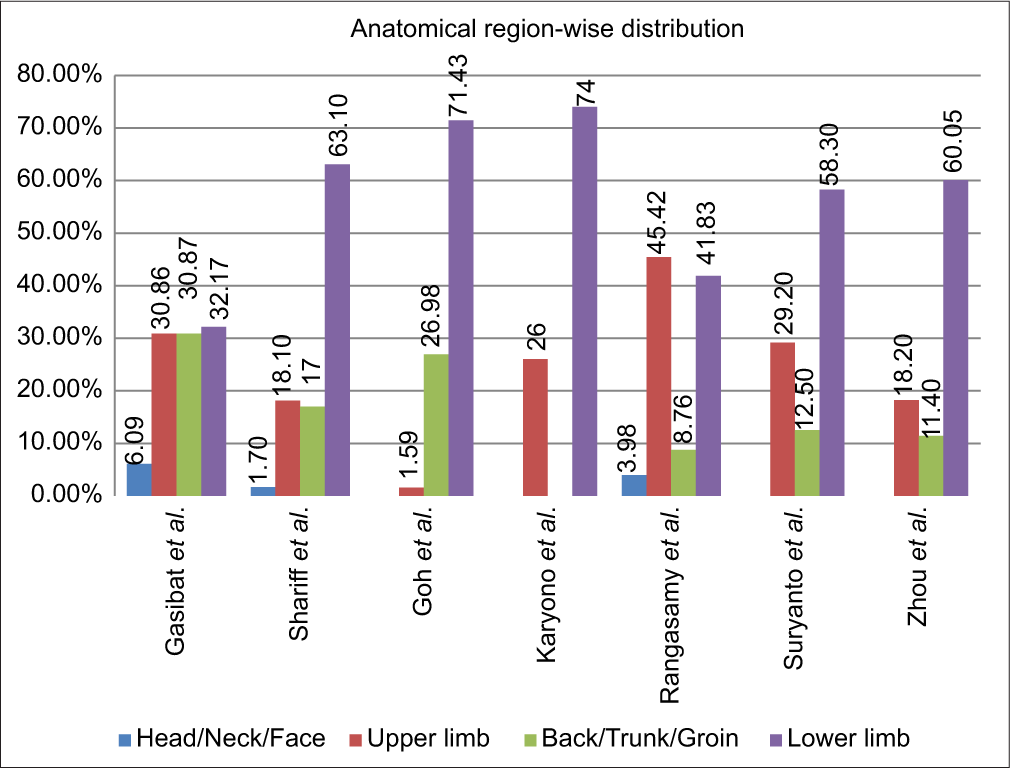
- Anatomical distribution of injuries (in percentage).
| Author | Total injuries | Head/neck/face | Upper limb | Back/trunk/groin | Lower limb |
|---|---|---|---|---|---|
| Gasibat et al. | 230 | Neck: 6.09% | Shoulder: 15.65%, Wrists/hand: 12.17% and elbow: 3.04%. | Lower back: 19.57%, Upper back: 11.3%. | Hips/thighs: 13.91%, Ankle: 10%, Knee: 8.26%. |
| Shariff et al. | 469 | Neck: 1.7% | UL : 18.1% | Back: 16.6%, Abdomen: 0.4%. | LL : 63.1% |
| Goh et al. | 63 | Shoulder: 1 (1.59%) | Back/Spine: 16 and Chest: 1 (26.98%) | Foot: 3, Ankle: 9, Leg: 8, Knee: 17, Thigh: 7, Gluteal: 1 (71.43%) | |
| Karyono et al. | 423 | 26% UL | 74% LL | ||
| Rangasamy et al. | 251 | Neck: 8, Face/Eye: 2 (3.98%) | Shoulder: 47, Elbow: 25, Wrist: 42 (45.42%) | Hip: 9, Back: 13 (8.76%) | Ankle: 65, Knee: 40 (41.83%) |
| Suryanto et al. | 24 | UL: 29.2% | Trunk: 12.5% | LL: 58.3% | |
| Zhou et al. | 554 | Shoulder: 8.1%, Elbow: 4.5%, Wrist: 3.4%, Upper arm: 2.2%. | Lower back: 6.5%, Groin: 4.9% | Ankle: 12.5%, Knee: 11.4%, Plantar: 10.1%, Toe: 5.8%, Quadriceps: 4.9%, Calf: 4.3%, Achilles tendon: 4.3%, Hamstring: 4%, Shin: 2.75%. |
UL: Upper limb, LL: Lower limb
Head/neck/face
The random-effects model, drawn from 3 studies, revealed a pooled prevalence of 1.76% for the Head/Neck/Face (HNF) (95% CI: 2.01–3.3; P = 0.027). The pooled estimate of effects in this meta-analysis showed substantial heterogeneity among studies (I2 = 96.64%, P < 0.001). The funnel plot, when visually inspected, suggested an asymmetry and demonstrated publication bias (Fail-safe n = 54, P < 0.001).
Upper limb
The random-effects model, drawn from 7 studies, revealed a pooled prevalence of 23.8% for the upper limb (95% CI: 13.4– 34.2; P < 0.001). The pooled estimate of effects in this meta-analysis showed substantial heterogeneity among studies (I2 = 97. 41%, P < 0.001). The funnel plot, when visually inspected, suggested an asymmetry and demonstrated publication bias (Fail-safe n = 1424, P < 0.001).
Back/trunk/groin
The random-effects model, drawn from 6 studies, revealed a pooled prevalence of 14.9% for the back/trunk/groin (95% CI: 6.9–23.0; P < 0.001). The pooled estimate of effects in this meta-analysis showed substantial heterogeneity among studies (I2 = 97. 92%, P < 0.001). The funnel plot, when visually inspected, suggested an asymmetry and demonstrated publication bias (Fail-safe n = 605, P < 0.001).
Lower limb
The random-effects model, drawn from 7 studies, revealed a pooled prevalence of 57.1% for the lower limb (95% CI: 45.4–68.8; P < 0.001). The pooled estimate of effects in this meta-analysis showed substantial heterogeneity among studies (I2 = 96.49%, P < 0.001). The funnel plot, when visually inspected, suggested an asymmetry and demonstrated publication bias (Fail-safe n = 6640, P < 0.001) [Figure 5].
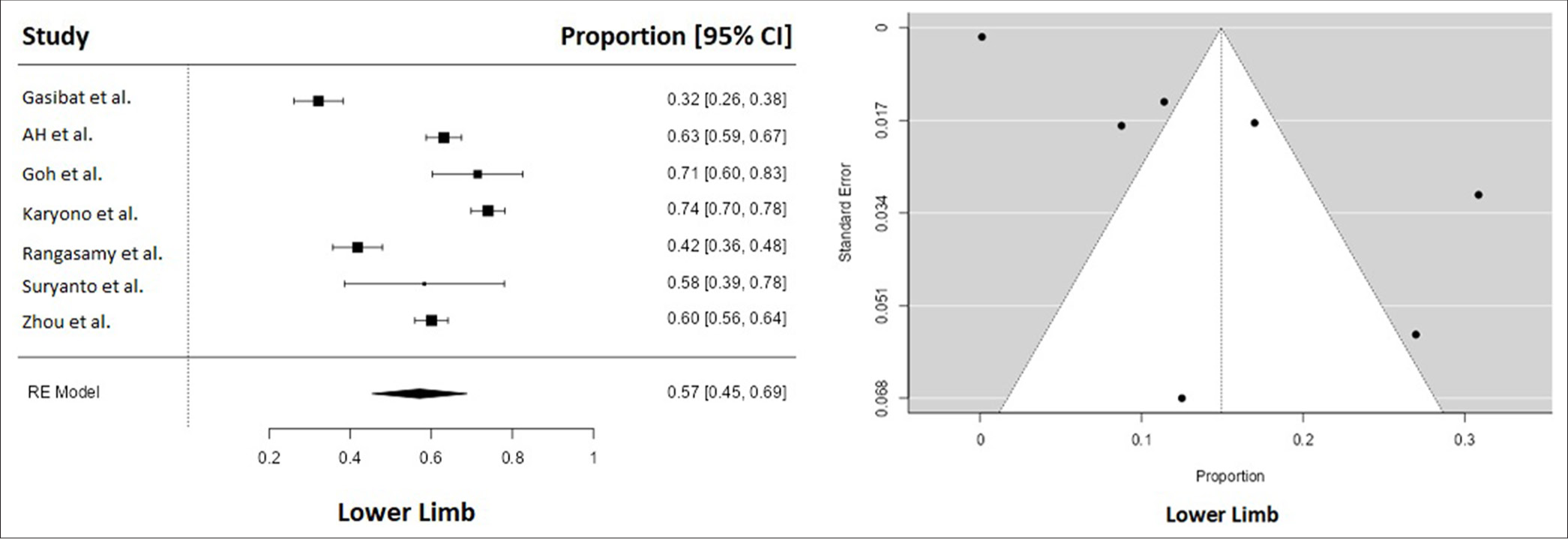
- Forest and funnel plot depicting lower limb injuries.
Distribution of overuse injuries
The random-effects model, drawn from 6 studies, revealed a pooled prevalence of 34.7% for the overuse injuries (95% CI: 15.8–53.6; P < 0.001). The pooled estimate of effects in this meta-analysis showed substantial heterogeneity among studies (I2 = 98.72%, P < 0.001). The funnel plot, when visually inspected, suggested an asymmetry and demonstrated publication bias (Fail-safe n = 1679, P < 0.001) [Figure 6].
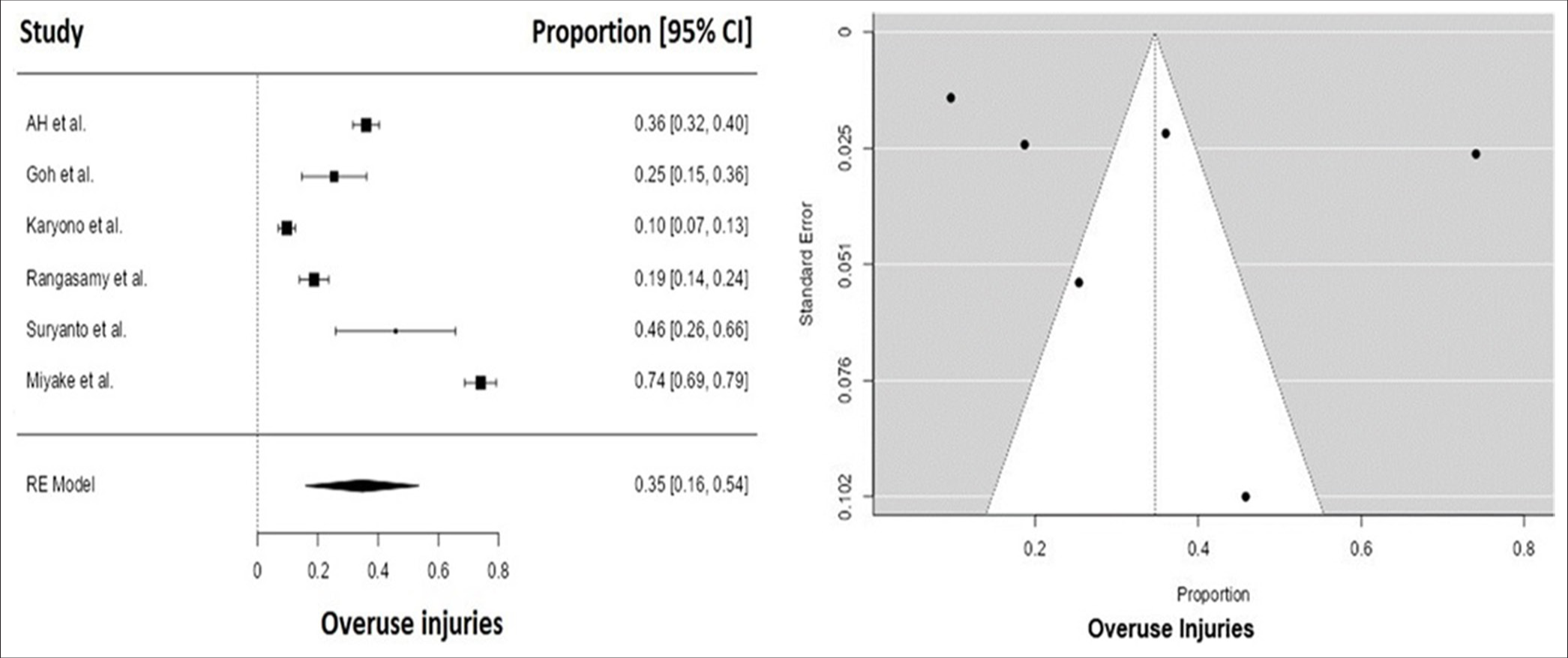
- Forest and funnel plot depicting overuse injuries.
Distribution on the basis of nature of injuries
The distribution of injuries, categorized according to their nature, was classified into four primary groups for comparative analysis: bone, ligament, muscle/tendon injuries, and soft tissue/skin injuries. One particular study[2] documented the highest proportion of bone injuries, i.e., 19.10%. Ligament injuries of 39.44%[7] were reported in one study. The other study reported the maximum muscle/tendon injuries of 30.92%[6] [Table 7].
| Author | Total Injuries | Bone | Ligament | Muscle/Tendon | Soft tissue/Skin | Others |
|---|---|---|---|---|---|---|
| Gasibat et al. | 230 | |||||
| Shariff et al. | 469 | 23 (4.9%) | 122 (26.01%) | 145 (30.92%) | 179 (38.1%) | |
| Goh et al. | 63 | 19.10% | 6.30% | 9.50% | 1.60% | |
| Karyono et al. | 423 | |||||
| Rangasamy et al. | 251 | 17 (6.77%) | 99 (39.44%) | 73 (29.08%) | 13 (5.18%) | 49 (19.52%) |
| Suryanto et al. | 24 | 8.30% | 12.50% | 50% | 12.50% | 16.70% |
| Zhou et al. | 554 |
Bone
The random-effects model, drawn from 4 studies, revealed a pooled prevalence of 8.28% for the bone (95% CI: 3.2–13.4; P = 0.001). The pooled estimate of effects in this meta-analysis showed substantial heterogeneity among studies (I2 = 79.89%, P = 0.036). The funnel plot, when visually inspected, suggested an asymmetry and demonstrated publication bias (Fail-safe n = 74, P < 0.001).
Ligament
The random-effects model, drawn from 3 studies, revealed a pooled prevalence of 26.9% for the ligament (95% CI: 12.4– 41.4; P < 0.001). The pooled estimate of effects in this meta-analysis showed substantial heterogeneity among studies (I2 = 92.94%, P < 0.001). The funnel plot, when visually inspected, suggested an asymmetry and demonstrated publication bias (Fail-safe n = 277, P < 0.001).
Muscle/tendon
The random-effects model, drawn from three studies revealed a pooled prevalence of 30.8% for the muscle/tendon (95% CI: 27.5–34.1; P < 0.001). The pooled estimate of effects in this meta-analysis showed no heterogeneity among studies (I2 = 0.05%, P = 0.142). The funnel plot, when visually inspected, suggested an asymmetry and demonstrated publication bias (Fail-safe n = 320, P < 0.001) [Figure 7].
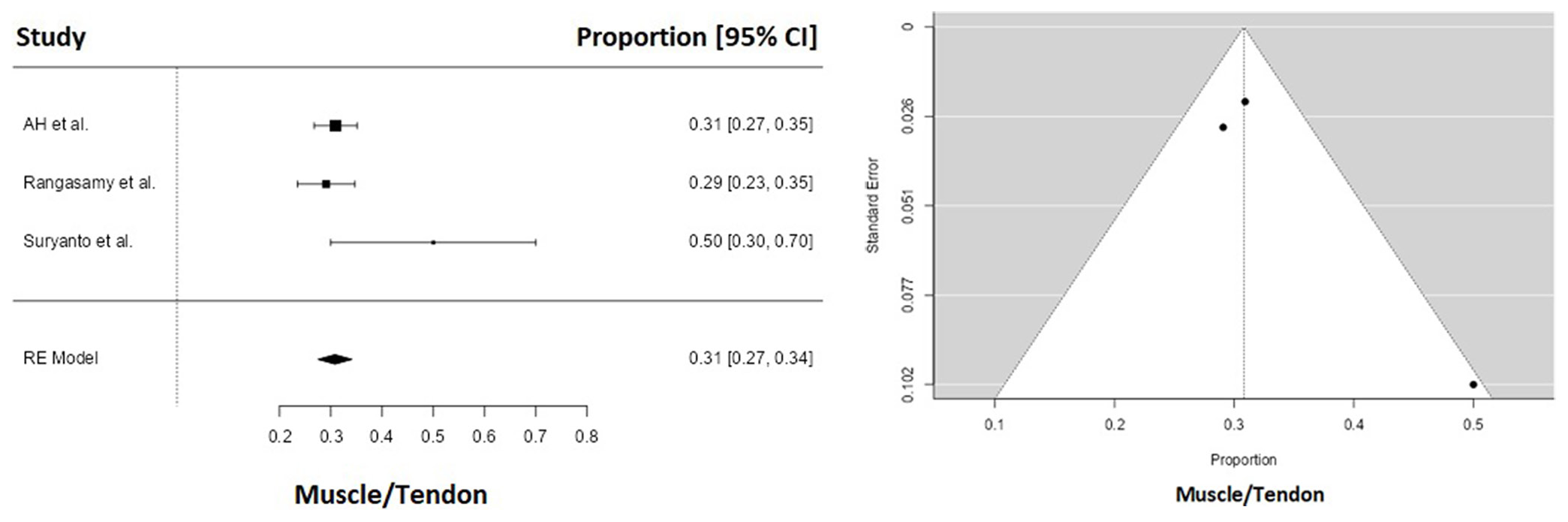
- Forest and funnel plot depicting muscle/tendon injuries.
Soft tissues/skin
The random-effects model, drawn from three studies, revealed a pooled prevalence of 6.72% for the soft tissue (95% CI: 2.9–10.6; P = 0.106). The pooled estimate of effects in this meta-analysis showed no heterogeneity among studies (I2 = 22.75%, P = 0.336). The funnel plot, when visually inspected, suggested an asymmetry and demonstrated publication bias (Fail-safe n = 22, P < 0.001).
DISCUSSION
Badminton is a sport that places significant biomechanical demands on its participants. The physical exertion required is intermittent, characterized by periods of high-intensity activity interspersed with very brief rest intervals. Despite its widespread popularity and extensive participation both recreationally and competitively, there exists a paucity of epidemiological studies on the sport. Moreover, the existing data are hindered by a lack of comparability, attributable to inconsistencies in injury definitions, variations in study design, and differing data collection methodologies.[10]
Badminton has been formally acknowledged as a leading core sport in Asia. Over the last 30 years, the continent has consistently cultivated numerous world-class athletes. As a non-contact sport, badminton demands jumps, lunges, and quick directional changes, along with rapid arm movements from various postural positions.[6] The epidemiology of badminton injuries is well-documented and demonstrates significant variability across different populations. Examining the epidemiology of injuries within a specific demographic is essential for comprehending their prevalence and severity, thus aiding in the formulation and execution of effective injury prevention strategies.[7]
Badminton, similar to other sports involving overhead motions such as tennis and baseball, requires rapid positional adjustments and dynamic movements, including lunges, jumps, twists, and swings. Due to the nature of badminton, it is essential to consistently coordinate the movements of all body joints. These actions involve weight shifting, upper limb rotation, trunk rotation, and instantaneous starting and stopping in response to receiving a shuttlecock from multiple directions.[8] However, given the insufficient allocation of dedicated medical personnel for certain teams and the inherent challenges associated with abstaining from practice and matches, it is essential that elite athletes engage in injury prevention programs. To effectively mitigate the risk of badminton injuries increasing in severity, we strongly recommend the implementation of a systematic injury prevention program specifically tailored to address chronic injuries.[9]
A standardized definition of badminton injuries should be implemented likewise other sports injury definitions, such as cricket[11] and football.[12] To mitigate the risk of injury and promote pain-free participation in badminton, it is essential to implement a preventive strategy beginning at the pre-adolescent stage. Future research must rigorously investigate the optimal training volume required to prevent pain and injuries associated with badminton among youth players. Therefore, it is crucial for forthcoming studies to focus on the physical fitness and motor skills specific to badminton in pre-adolescent and adolescent athletes. Acquiring a comprehensive understanding of the most common types of injuries, alongside identifying individuals at increased risk, are vital steps toward developing an effective injury prevention program. Such a program would be indispensable in sustaining these young athletes’ performance levels, thereby ensuring their potential as future professional competitors and valuable national assets.[1]
It is essential to acknowledge that impact forces and knee movements are crucial in understanding the kinetic characteristics of the lower extremities during a lunge movement. However, there has been a notable increase in the proportion of upper limb injuries in recent years, which may be attributed to heightened shot intensity and smash speed. Moreover, these injuries are more prevalent at the beginning of play and are frequently associated with perceptions of fatigue. Improving warm-up protocols to ensure optimal muscle activation and avoiding overtraining scenarios could play a significant role in mitigating the occurrence of such injuries.[13] Numerous studies have indicated a significant correlation between dysfunction in the trunk or lower extremities and injuries to the elbow and shoulder in adult overhead athletes. Considering the rigorous demands of such sports and the well-documented patterns of overuse injuries across various levels and genders, there is a strong rationale for integrating a rotation of sports into training programs, especially for adolescent athletes.[10]
Inadequate training methodologies and numerous risk factors may predispose athletes to lower limb overuse injuries impacting the bone, such as stress reactions and stress fractures. It is essential for badminton coaches and trainers to consider these findings seriously and contemplate modifications to the training workload of badminton players. Such adjustments are crucial to facilitate physical recovery and disrupt the repetitive cycle that leads to overuse injuries. While many overuse injuries tend to resolve on their own, they can lead to an increase in hospital visits and have the potential to progress into chronic pain conditions.[14]
Anatomical region
The game is fundamentally focused on speed and deception, marked by sudden jerking movements and swift footwork. This combination of repetitive maneuvers places considerable stress on both the upper and lower extremities, thereby increasing the risk of acute and chronic injuries of varying severity. Simultaneously, the repeated motion involved in overhead strokes and short-hitting actions subjects the upper extremity, particularly the shoulder, to repetitive rotational stress. In addition, rapid and frequent lunges and jumps in badminton have been identified as contributing factors to significant impact loading on players’ lower extremities, consequently leading to overuse knee injuries.[6]
Furthermore, Sekiguchi et al.,[15] observed that pain in the elbow and/or shoulder more commonly co-occurs with pain in the back and hip, as opposed to pain in the knee and foot. The associations between trunk pain (encompassing the back and hip) and discomfort in the elbow and shoulder exhibit a significantly stronger correlation than those involving the lower extremities, such as the knee and foot.
Our results confirmed that the majority (57.1%) of injuries were lower limb injuries.
In a 12-month prospective study conducted at Institute of Sport, Expertise and Performance (INSEP) in France,[13] involving the international elite badminton players of the federal training group, the prevalence of lower limb injuries was the most frequent, i.e., 54.3%.
In a cross-sectional study conducted by the Badminton World Federation (BWF) in the United Kingdom,[16] the prevalence of lower limb injuries was 67.31%.
In a cross-sectional study drawn from the 2018 BWF European Senior Championships,[17] the prevalence of lower limb injuries was 40.7%.
Overuse injuries
Epidemiological studies conducted in hospital settings, through questionnaires, and through physiotherapy assessments have consistently identified overuse injuries of the lower limb as one of the common types of injury associated with badminton. The correlation between elevated knee flexion/extension moments and increased quadriceps and tibial shear forces indicates that athletes lacking skill may be at an elevated risk for such injuries. The intrinsic loading characteristics of badminton on the lower limbs appear to contribute to overuse injuries occurring approximately 3 times more frequently than traumatic injuries. Notably, lunges – a common movement in badminton – are particularly linked to a heightened risk of overuse injuries, including patellar and Achilles tendinopathies.[18]
Our study reported 34.7% of the pooled prevalence of overuse injuries.
In a 12-month prospective study conducted at INSEP in France,[13] involving the international elite badminton players of the federal training group, the prevalence of overuse injuries was 62.9%.
Jørgensen and Winge[19] reported that >74% of badminton injuries were overuse injuries.
Nature of injury
Regular loading activities lead to modifications in the structural and mechanical properties of athletes’ tendons and muscles. The sudden and frequent acceleration and deceleration movements characteristic of badminton place a considerable eccentric load on the lower extremities, consequently heightening the risk of strains, sprains, and ligament injuries.[20]
Our study reported no heterogeneity in the specific nature of injuries due to less number of studies included in our review. In a cross-sectional study drawn from the 2018 BWF European Senior Championships,[17] muscle injuries were the most common, i.e., 39.1%, which is similar to our pooled prevalence of muscle injuries, i.e. 30.8%.
Incidence proportion of injuries
In our review, pooled data of the incidence proportion of injuries were reported to be 48.3%.
In a cross-sectional study conducted by the BWF in the United Kingdom,[16] the incidence proportion of injury was found to be 37.61%.
In a retrospective study conducted on the patients of Badminton-related acute injuries admitted to the Emergency Department of Hospital Sud in France,[21] the incidence proportion of injuries was reported to be 96.43%.
In a study conducted on regular badminton players in France,[22] the incidence proportion of injuries was found to be 66.37%.
In the realm of sports, particularly in badminton, the need for standardized definitions of injury is paramount. Currently, varying interpretations and classifications of injuries can lead to inconsistencies in treatment protocols, reporting practices, and injury prevention strategies. Standard injury definitions and injury reporting formats have been adopted in sports such as cricket[11] and football.[12] Establishing a set of standard definitions for badminton injuries would facilitate clearer communication among coaches, medical personnel, and players regarding the nature and severity of injuries sustained during play. Overuse injuries among badminton players are prevalent and frequently overlooked, which may affect their performance. As the prevalence of such injuries continues to rise, it becomes imperative to adopt a more proactive approach in their identification and treatment. Addressing overuse injuries with a focus on improved determination through advanced diagnostics and education will be essential for promoting the long-term health and performance of players.
Limitations
In the studies we included, there was an absence of a standardized injury definition and documentation methods. Furthermore, there was no consistent protocol for reporting injury patterns, identifying mechanisms, or calculating injury rates.
In addition to the limitations inherent in the included studies, it is imperative to acknowledge the constraints of the review process itself when interpreting the results. The search strategy was intentionally broad to encompass all original studies related to badminton. Nevertheless, there remains a possibility that significant studies addressing various sports or injuries may have included data on badminton within a subgroup analysis.
CONCLUSION
Badminton is a popular sport in the Asian region, with a significant following and participation. The inconsistent methodology employed across various studies is a significant cause for concern. It is imperative that researchers and policymakers take immediate action to address this critical issue. The lower extremities were predominantly the injured regions. Comprehensive studies involving larger sample sizes, standardized methodologies, and the consideration of multiple variables and factors are required to achieve a more complete and accurate representation of the problem. Further research is warranted to explore the long-term injury consequences and the variations in playing styles between elite and recreational players. Elite players often engage in rigorous training regimens and compete at higher intensities, which may predispose them to specific injuries that differ from those experienced by recreational players who typically participate at a more moderate level. Understanding these injuries is crucial for developing targeted injury prevention strategies tailored to different levels of play.
Author contributions
PS and NS: Writing - review and editing, writing - original draft, methodology, formal analysis, data curation, and conceptualization; KK: Supervision, designing search strategy, and database search; SM: Statistical analysis.
Ethical approval
The study was approved by the Institutional Review Board, approval number, IEC code: 2022-180-EMP-129, dated January 23, 2023.
Declaration of patient consent
Patient’s consent not required as there are no patients in this study.
Conflicts of interest
There are no conflict of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Incidence and risk factors for musculoskeletal injuries among Indonesian junior badminton athletes during a national elite championship. Acta Med Philippina. 2022;56:37-41.
- [CrossRef] [Google Scholar]
- Badminton injuries in youth competitive players. J Sports Med Phys Fitness. 2013;53:65-70.
- [Google Scholar]
- Musculoskeletal disorders among elite junior Malaysian badminton players. Sport Sci. 2022;15:44-50.
- [Google Scholar]
- Risk factors for lower extremity injuries in young badminton players. Sci Med. 2018;28:28939.
- [CrossRef] [Google Scholar]
- A survey on types of injuries in Indonesian recreational badminton players. Intern J Human Mov Sports Sci. 2022;10:49-53.
- [CrossRef] [Google Scholar]
- Musculoskeletal injuries among Malaysian badminton players. Singapore Med J. 2009;50:1095-7.
- [Google Scholar]
- Risk prediction of injury among recreational badminton players in India. Indian J Orthop. 2022;56:1378-84.
- [CrossRef] [PubMed] [Google Scholar]
- The characteristics of badminton-related pain in pre-adolescent and adolescent badminton players. Children (Basel). 2023;10:1501.
- [CrossRef] [PubMed] [Google Scholar]
- A prospective epidemiological study of injuries in Japanese national tournament-level badminton players from junior high school to university. Asian J Sports Med. 2016;7:e29637.
- [CrossRef] [PubMed] [Google Scholar]
- Badminton injuries in elite athletes: A review of epidemiology and biomechanics. Indian J Orthop. 2020;54:237-45.
- [CrossRef] [PubMed] [Google Scholar]
- International consensus statement on injury surveillance in cricket: A 2016 update. Br J Sports Med. 2016;50:1245-51.
- [CrossRef] [PubMed] [Google Scholar]
- Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Br J Sports Med. 2006;40:193-201.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiology of Injuries in elite badminton players: A prospective study. Clin J Sport Med. 2021;31:e473-5.
- [CrossRef] [PubMed] [Google Scholar]
- Influence of ankle injury on subsequent ankle, knee, and shoulder injuries in competitive badminton players younger than 13 years. Orthop J Sports Med. 2022;10:1-6.
- [CrossRef] [PubMed] [Google Scholar]
- Coexistence of trunk or lower extremity pain with elbow and/or shoulder pain among young overhead athletes: A cross-sectional study. Tohoku J Exp Med. 2017;243:173-8.
- [CrossRef] [PubMed] [Google Scholar]
- Training and injuries among world elite junior badminton players-Identifying the problems. Asia Pac J Sports Med Arthrosc Rehabil Technol. 2021;26:21-6.
- [CrossRef] [PubMed] [Google Scholar]
- Incidence of injuries among amateur badminton players: A cross-sectional study. Medicine (Baltimore). 2020;99:e19785.
- [CrossRef] [PubMed] [Google Scholar]
- Differences in tendon properties in elite badminton players with or without patellar tendinopathy. Scand J Med Sci Sports. 2013;23:e89-95.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiology of badminton injuries. Int J Sports Med. 1987;8:379-82.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiological patterns of alternative racquet-sport injuries in the United States, 1997-2016. Orthop J Sports Med. 2018;6:1-7.
- [CrossRef] [PubMed] [Google Scholar]
- Acute injuries in Badminton from 10 to 66 years of age: An epidemiological study of 140 cases among all types of practice. Eur J Orthop Surg Traumatol. 2023;33:1945-51.
- [CrossRef] [PubMed] [Google Scholar]
- Injuries in French and Chinese regular badminton players. Sci Sports. 2018;33:145-51.
- [CrossRef] [Google Scholar]




