
Translate this page into:
Can the ideal femoral tunnel position be achieved by modified transtibial technique of anterior cruciate ligament reconstruction using bone patellar bone graft? – A prospective study
 , Parthiban Jeganathan1, Suresh Perumal1, Vivek Kumar Gupta1, Vignesh Murali1, Arumugam Sivaraman1
, Parthiban Jeganathan1, Suresh Perumal1, Vivek Kumar Gupta1, Vignesh Murali1, Arumugam Sivaraman1
*Corresponding author: Harish Mahesan, Department of Orthopaedics, Sri Ramachandra Centre for Sports Science, Sri Ramachandra Institute of Higher Education and Research, Chennai, Tamil Nadu, India. harishmahesan@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Mahesan H, Jeganathan P, Perumal S, Gupta VK, Murali V, Sivaraman A. Can the ideal femoral tunnel position be achieved by modified transtibial technique of anterior cruciate ligament reconstruction using bone patellar bone graft? – A prospective study. J Arthrosc Surg Sports Med. doi: 10.25259/JASSM_59_2024
Abstract
In the transition from isometric to anatomical anterior cruciate ligament (ACL) reconstruction, the transportal technique of ACL reconstruction has become the widely used method. However, with the difficulty in bone patellar bone (BTB) graft passage and technical demand, transtibial is gaining popularity over the transportal technique. For achieving a femoral tunnel to be centered in the ACL attachment site using the traditional transtibial approach of ACL reconstruction, a shorter tibial tunnel becomes inevitable. By adopting a modified transtibial approach for ACL reconstruction with a BTB graft, the study intends to analyze the accuracy of the femoral tunnel. Thirty four patients who underwent single-bundle ACL reconstruction with BTB graft using the modified transtibial technique in a single center were included in the study. The femoral tunnel position was determined with a computed tomography scan using the quadrant method. The results were compared with that of cadaveric study and transportal technique. The tibial tunnel angulation in the coronal plane and intraarticular aperture location was measured for standardization of the technique. The mean distance of the femoral tunnel from the posterior condylar surface (t) was 33 +/- 6.8, and from the notch (h) was 21 +/- 5.2. On comparing the horizontal distance (t) obtained with that of the transportal technique (P = 0.001; 95% confidence interval (CI); difference -10) and cadaveric study (P = 0.016; 95% CI; difference -5) by the analysis of variance (ANOVA) post hoc test, p-value was found to be significant. Similarly, on comparing the vertical distance (h) with that of the transportal technique (P = 0.9; 95% CI; difference 2), P value was found to be not significant. The drawback of the conventional transtibial approach is thus addressed by our modified transtibial technique of ACL repair with BTB graft, which makes the femoral tunnel nearly anatomical and comparable to the tunnel location achieved by the transportal technique.
Keywords
Anterior cruciate ligament reconstruction
Bone patellar bone graft
Femoral tunnel
Modified transtibial technique

INTRODUCTION
The commonly used autografts for anterior cruciate ligament (ACL) reconstruction are hamstring and bone patellar bone (BTB) grafts.[1] In the transition from isometric to anatomical ACL reconstruction, the transportal method of ACL reconstruction has become the most preferred technique, as it offers better obliquity of the femoral tunnel and restores the native femoral footprint of the ACL compared to the traditional transtibial method.[2] Thus, the ACL reconstruction with a hamstring graft is usually done by the transportal technique.
It has long been known that graft alignment, both coronal and sagittal, plays a crucial role in the rotational and anteroposterior stability of ACL reconstruction. Even though isometric femoral tunnel positioning and a vertical graft orientation can effectively control anterior tibial translation, patients frequently experience persistent rotational instability and a pivot shift after surgery that prevents them from returning to their pre-operative level of athletic activity and contributes to graft failure.[3-5] This has led to the usage of BTB grafts in high-demanding patients and revision cases. Although ACL reconstruction with BTB graft can be done by both the transtibial and transportal methods, the transtibial method remains the widely preferred technique. This is because the passage of BTB graft through the femoral tunnel becomes more challenging in the case of the transportal technique due to the obliquity of the femoral tunnel. Moreover, while placing the femoral tunnel through the transportal technique, the possibility of damaging the medial femoral condyle makes it technically challenging.[6]
However, non-anatomical femoral tunnel placement is not very uncommon in both the transtibial and transportal methods of ACL reconstruction. In the aim of creating a femoral tunnel in the center of the ACL footprint following a transtibial approach, the guide pin is placed closer to the joint line on the tibial side, resulting in a short tibial tunnel, which, in turn, leads to the graft failure.[7] The conventional transtibial technique places the femoral tunnel in a higher position than the desired point. Considering these issues, surgeons now prefer the transportal method of ACL reconstruction.
The study intends to resolve this difference of opinion by analyzing the femoral tunnel position from the described modified transtibial technique of ACL reconstruction using BTB graft and to assess the variations in femoral tunnel position in a native ACL, transtibial method and transportal method.
MATERIALS AND METHODS
Thirty-four patients who were diagnosed with ACL rupture and underwent single-bundle ACL reconstruction with BTB autograft were included in the study. All the surgeries were done by a single arthroscopy fellowship-trained surgeon. All patients were clearly explained about their participation in the study, and also, written and informed consent was obtained for further radiological assessment. Ethical committee clearance was obtained before starting the study (ref no: CSP-MED/24/MAY/80/144). The femoral tunnel was drilled by the modified transtibial technique in all the patients. 3D computed tomography (CT) and X-ray were taken postoperatively after one month to evaluate the femoral tunnel position.
The femoral tunnel position was calculated using the quadrant method. Radiological measurements were calculated with the help of a musculoskeletal radiologist and an arthroscopy surgeon, and interobserver and intraobserver correlation coefficients were calculated to standardize the findings. Unlike the original method, where a plain X-ray was used, a 3D CT image of the lateral femoral condyle at the level of the intercondylar notch was used for the quadrant method.[8]
The center point of the femoral tunnel is point K. Distance T represents the entire sagittal diameter of the lateral femoral condyle, and distance H represents the intercondylar notch height. Distance A represents the distance between point K and the deep subchondral contour of the lateral femoral condyle, whereas distance B represents the distance between point K and the maximum intercondylar notch height. “T” and “H” are A and B expressed as a percentage of T and H, respectively [Figure 1].
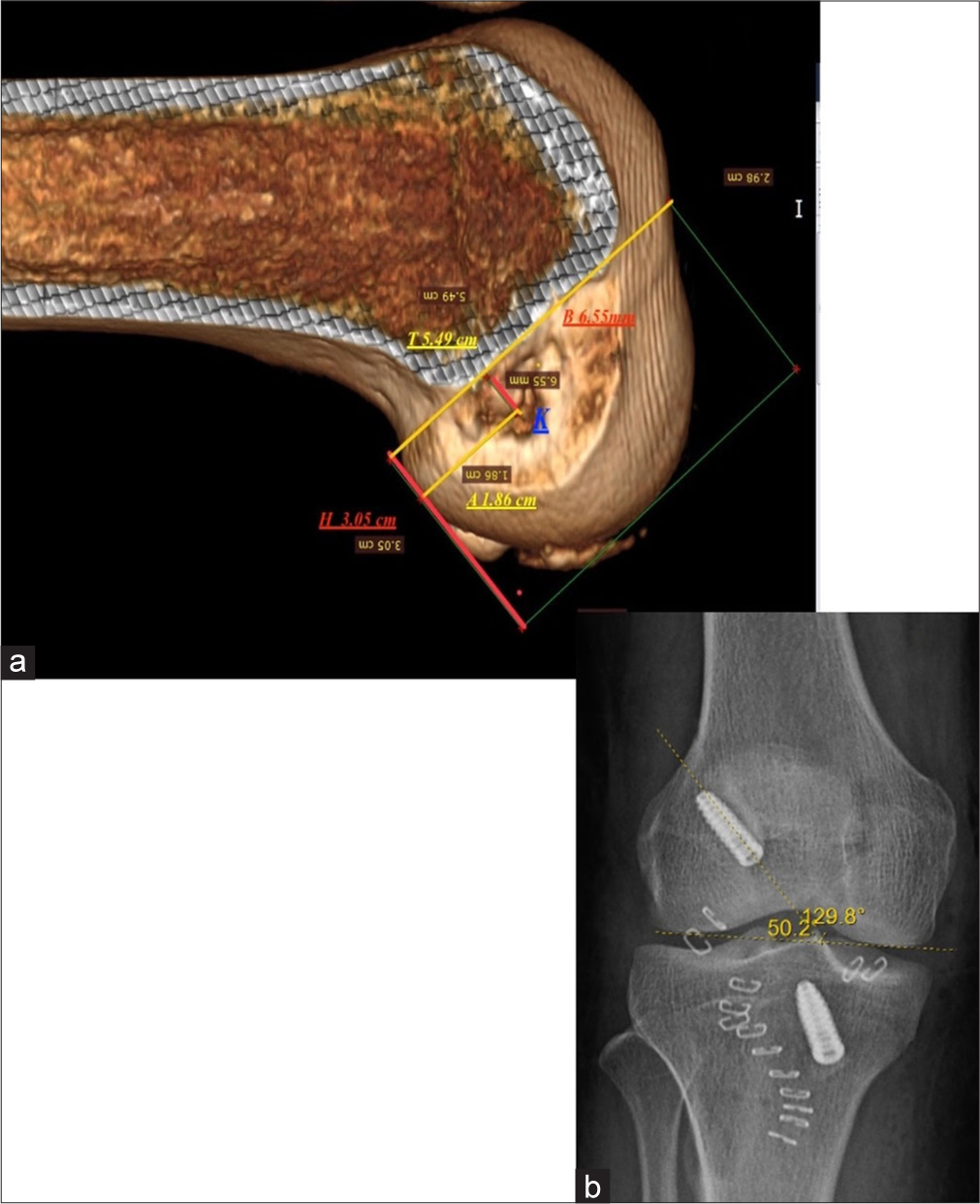
- (a) 3D computed tomography, showing the quadrants method for determining femoral tunnel position, where t (horizontal) = A (1.86 cm)/T (5.49 cm) × 100 and h (vertical) = B (6.55 mm)/H (3.05 cm) × 100. (b) Femoral tunnel angle in coronal plane measured as 50.2° showing adequate obliquity.
A post-operative X-ray was taken and was used to note the obliquity of the tunnel. The angle formed by the tunnel with the tangential line drawn along the most convex points of the femoral condyle was noted. These values were compared with the anatomical ACL attachment site as measured by the quadrant method.[9,10]
For the standardization of the technique, tibial tunnel position and angulation were measured. A reference standard technique was used to measure the intra-articular aperture positioning after ACL reconstruction. Here, a 3D CT axial image of the tibia was used with a rectangular grid drawn along the borders of the anterior, posterior, medial, and lateral cortices of the tibia. The center of the tibial tunnel was marked, and its distance was measured from the anterior and medial borders. The tibial tunnel angulation in the coronal plane was measured from the horizontal reference line drawn along the tibial plateau in the post-operative X-ray [Figure 2].
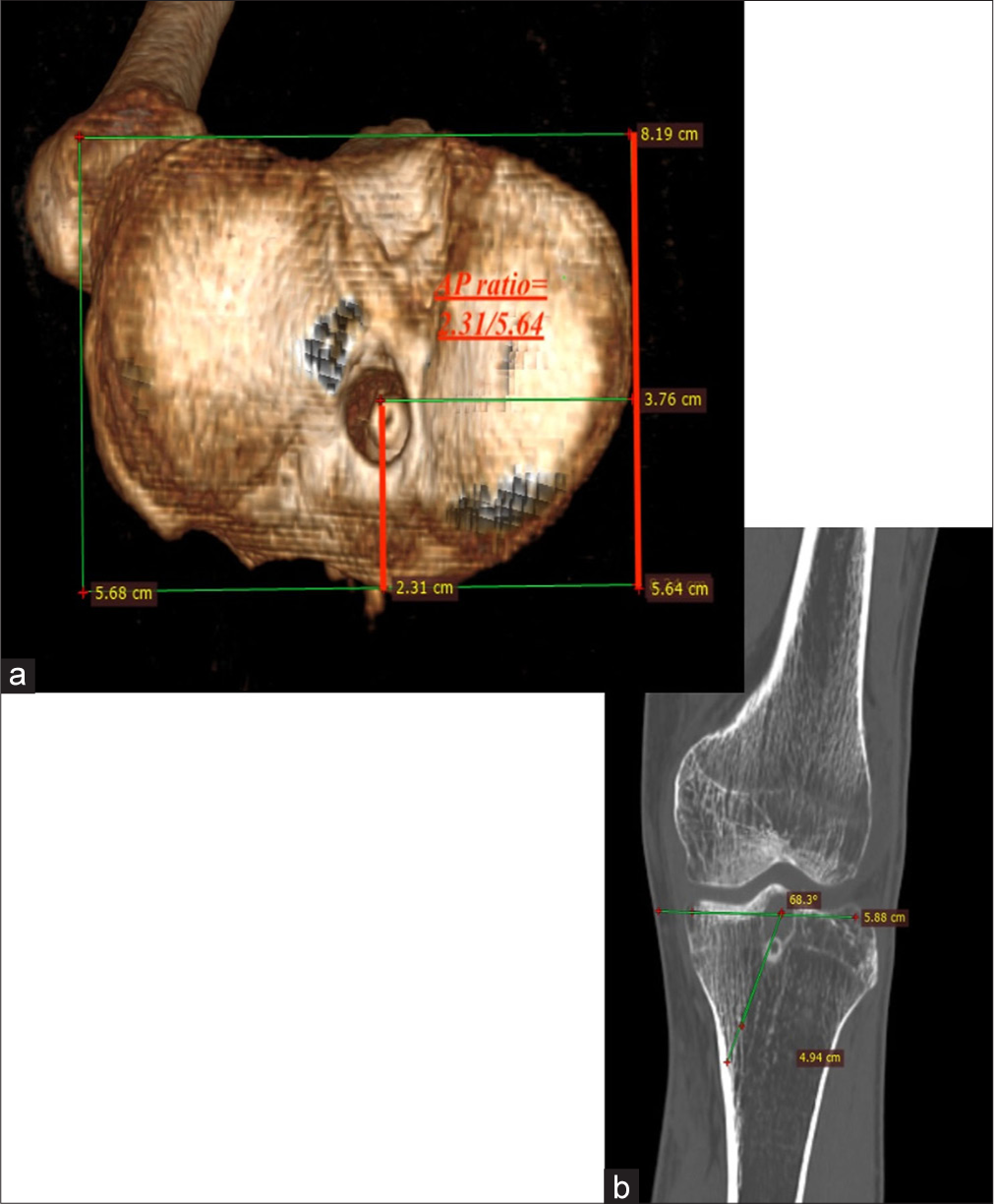
- (a) Intra-articular aperture position of tibial tunnel calculated by reference method in 3D computed tomography, showing tunnel located at 40.95% (2.31/5.64 × 100) of maximum A width of tibia. (b) Tibial tunnel angulation in coronal plane as measured is 68.3°.
SURGICAL TECHNIQUE
All the patients underwent surgery under general anesthesia and tourniquet control. After confirmation of ACL tear with diagnostic arthroscopy, the BTB graft was harvested using the mobile window technique as already described in our publication.[11] Using a small oblique incision directed medially, a rectangular mobile window was created with adequate subcutaneous dissection. Paratenon was incised, and the middle third of the patellar tendon was incised with the knee in 100-120° flexion. With 30° knee flexion and retraction distally, a tibial bone plug with tongue was harvested. Similarly, with the knee in extension, a patella bone plug was harvested. The harvested graft was prepared, with the tibial side measuring 11 mm and the femur side (patella) measuring 10 mm in width.
The intercondylar ridge and the posterior cortex of the femur are visualized by clearing the soft tissue. The remaining part of the ACL was preserved. The bony landmark of the ACL was made with the help of a microfracture awl through the anteromedial portal as a reference point. The tibial tunnel was prepared with the help of a jig. The starting point of the tunnel was made a few millimeters medial to the usual method (lateral to the lateral border of the superficial medial collateral ligament [MCL]); however, further reaming encroaches on the superficial MCL. Another landmark considered for placing the tibial guide wire is the midpoint of the tibial tubercle and the posterior border of the tibia. This allows the desired angulation for aiming the center of the femoral footprint through the posterior margin of the tibial ACL footprint. The desired point for the femoral tunnel is marked with the help of a microfracture awl. The posterior offset was passed through the tibial tunnel toward the impression marked with an awl and held in internal rotation such that the guide wire passed through the offset and emerged closer to it. A guide wire was drilled through the opposite cortex and exchanged with a flexible guide pin. A flexible femoral reamer was used to ream the femoral tunnel across the flexible guide wire with the knee in 90° flexion. Notcher was used superiorly along the tunnel. BTB graft was passed guided into the femoral tunnel with the help of a probe such that the cortical aspect of the patellar bone plug faces superiorly to engage the interference screw. Graft was fixed on either side with interference screws [Video 1 and Figure 3].
Video 1:
Video 1:Modified transtibial technique.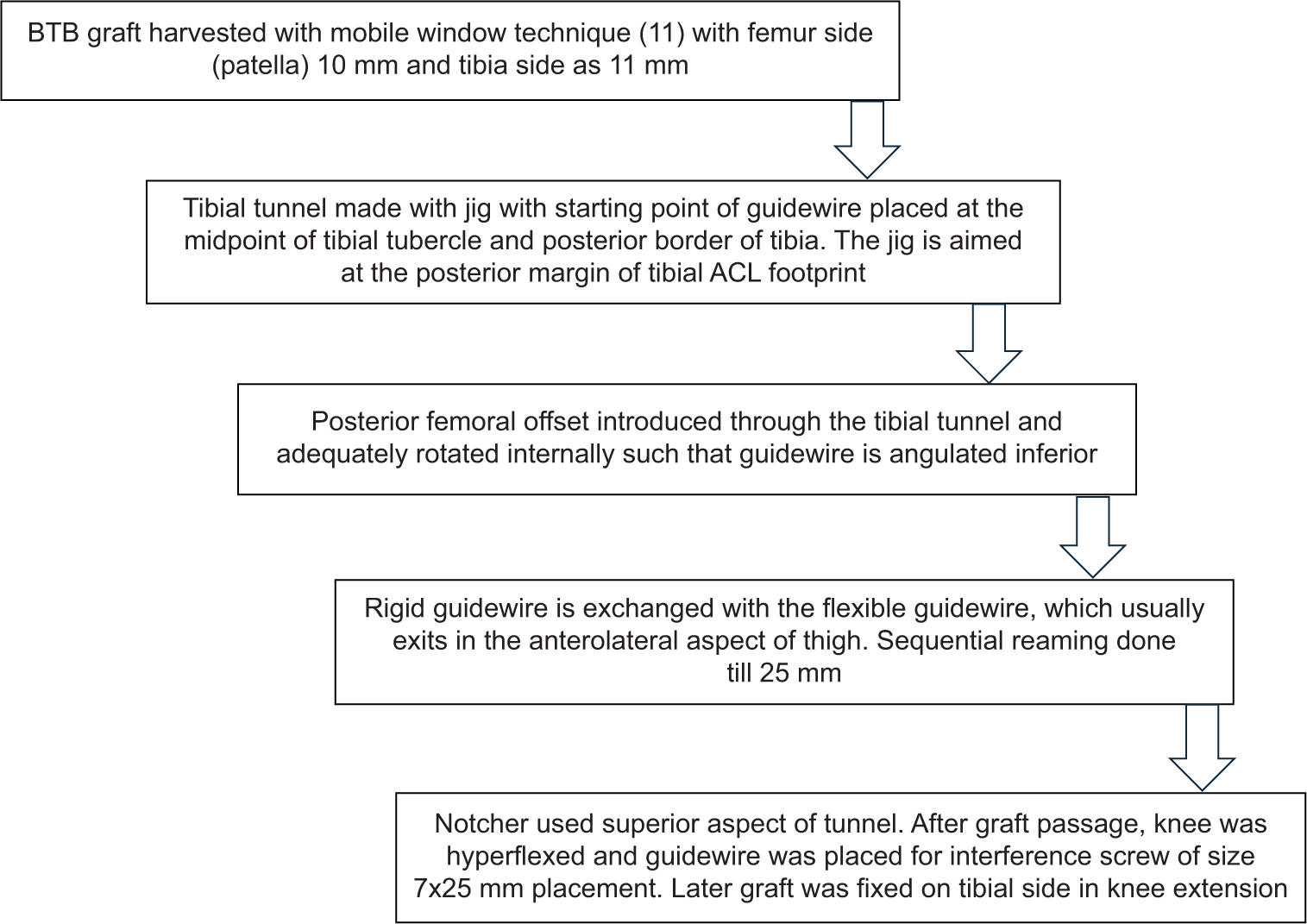
- Surgical technique. BTB: Bone patellar bone, ACL: Anterior cruciate ligament
In contrast to the traditional transtibial technique, the tibial tunnel starting point is made a few millimeters medial than the usual preferred point, in addition to an 11 mm tibial tunnel to angulate the guide wire, and the use of a flexible reamer and posterior offset helps to place the femoral tunnel in an ideal position [Figure 4].

- Flexible guide wire, flexible reamer, and posterior offset.
RESULTS
Thirty-four patients, after giving consent, who underwent ACL reconstruction with BTB graft using modified transtibial technique and had completed the follow-up with CT scan and post-operative X-ray were included in the study. All the patients were involved in sporting activity/high demanding activity. Out of 34 patients, 32 patients were male, and three patients were female. The mean age of the patient was 32.2 years (19–43 years). Twenty-two patients had noncontact twisting injuries while playing sports, ten patients had road traffic accidents, and other injuries in two patients. Of the 34 patients, 27 patients had isolated ACL injuries, six patients had associated meniscal injuries, and one patient had associated MCL injury.
All the radiological measurements were done by a musculoskeletal radiologist and an arthroscopy surgeon separately. Each variable was done twice by both observers. When the average of both assessments was obtained, interrater reliability was observed. The interobserver correlation intraclass correlation coefficient was 0.87, and the intraobserver correlation coefficient was 0.95 and 0.93.
The mean angle which the tibial tunnel made in reference to the tibial plateau was noted as 64.9°. The intra-articular aperture of the tunnel, as measured by the reference method, was 41.89% of the anteroposterior length and 42.15% of the mediolateral length [Table 1].
| Our results (%) | Other studies (%) | |
|---|---|---|
| Intra-articular aperture anteroposterior location | 41.89±5 | 44 |
| Tibial tunnel angle in coronal plane | 64.9±3.5 | 65–72 |
With this standardization of the tibial tunnel, the femoral tunnel position was analyzed in CT. The mean distance of the femoral tunnel from the posterior condylar surface – horizontal distance (t) was 33 ± 6.8, and from the notch, vertical height (h) was 21 ± 5.2. The mean femoral tunnel angulation measured in post-operative X-ray was 48.4 ± 4°, which was comparable to that of other studies.[12]
These results of the same were compared with the femoral tunnel position as analyzed by quadrant method in a cadaveric study[13] and a transportal technique study[14] using semitendinosus and gracilis graft using analysis of variance (ANOVA) post hoc test. The variance is similar in all the groups. Since the raw data of the other studies are not available for calculating the assumption, we assume that there is homogeneity of variants.
On comparing the horizontal distance (t) obtained with that of the transportal technique (P = 0.001; 95% confidence interval [CI]; difference −10) and cadaveric study (P = 0.016; 95% CI; difference −5) by ANOVA post hoc test, P-value was found to be significant.
Similarly, on comparing the vertical distance (h) with that of the transportal technique (P = 0.9; 95% CI; difference 2), the P value was found to be not significant [Table 2].
| Our results (%) | Transportal technique (Li et al.) (%) | Cadaveric study (Kim et al.) (%) | P-value 95% CI | Significance | |
|---|---|---|---|---|---|
| t (horizontal) | 34.87±6 | 24.2±6.86 | 29.5±2.8 |
P=0.001 P=0.016 |
Significant; Posterior placed tunnel and comparable to transportal technique and native ACL. |
| h (vertical) | 21±5 | 21.16±5.14 | 38.5±3.2 |
P=0.001 P=0.9 |
Significant; near anatomical. Not significant; adequately low and comparable femoral tunnel to transportal technique |
ACL: Anterior cruciate ligament, CI: Confidence interval
DISCUSSION
The position of the femoral and tibial tunnels plays a pivotal role in the success of an ACL reconstruction. To respect the isometry and prevent excursion of the ACL graft, non-anatomic isometric ACL reconstruction was extensively studied.[15] However, high femoral tunnel placement (11 o’clock and 12 o’clock position) does not resist the rotatory load.[16] Thus, the surgical technique shifted toward placing the graft lower and near the anatomical footprint of the native ACL (10 o’clock position).
Although the transportal technique is commonly used in achieving the low placement of the femoral tunnel, it comes with the technical difficulties of maneuvering the BTB graft into the oblique femoral tunnel, maintaining hyperflexion of the knee from guide wire placement to reaming, and avoiding the iatrogenic damage to the medial femoral condyle while reaming the femoral tunnel. A multicentric study comparing transportal with transtibial technique showed a higher revision rate with the transportal technique, due to increased complexity of the procedure.[17] However, the rate of non-anatomic femoral tunnel remains comparable in both transtibial and transportal techniques, highlighting no relationship between the drilling technique and tunnel position.[18] Consequently, research into the transtibial tunnel and methods of creating an anatomical femoral tunnel through the tibial tunnel began. The study aims to modify the transtibial technique with the help of post-operative CT imaging for analyzing the femoral tunnel position.
There are several described modified transtibial techniques, such as the triangular funnel-shaped bony trough employed to slip the guide wire from eccentric to the anticipated anatomic center.[12] However, it may cause breakage of the guide wire while reaming or a shallow tibial tunnel if not careful. To overcome these difficulties, we have used a flexible reamer and guide wire to create the desired trajectory of the femoral tunnel. Although both the flexible and rigid reamers allow for reproducible anatomic femoral tunnels, the flexible reamer helps us to achieve longer and more anteverted femoral tunnels compared to the rigid reamer.[19]
Unlike the usual graft diameter, a femoral tunnel size of 10 mm and a tibial tunnel size of 11 mm is preferred so that the guide pin aimed from the tibial end can be adequately angled to reach the desired position on the femoral condyle. In addition to this, the usage of posterior femoral offset provides further leverage to place the guidewire lower and more posterior than the usual transtibial femoral tunnel by internally rotating the offset.
The t-value, as obtained using the modified transtibial technique, on comparison with the transportal technique[14] and cadaveric study,[13] was found to be statistically significant. Although significant, the femoral tunnel is placed adequately posterior (deep) and comparable to other studies. Similarly, the h value as obtained by the modified transtibial technique is statistically not significant compared to that of the transportal technique, showing that the femoral tunnel is adequately low (inferior), similar to that made by the transportal technique. However, the h value of the femoral tunnel using the modified transtibial technique is less than that of the native ACL seen in the cadaveric study, making it near anatomical (like the transportal technique). Although transportal and transtibial tunnels are inherently different, the medialized tibial tunnel, which is angulated towards the posterior margin of ACL tibial footprint (close to the tibial plateau), helps modified transtibial technique achieve a low and posterior femoral tunnel. In single-bundle ACL reconstruction, irrespective of the technique used, the femoral tunnel position is aimed at the anteromedial bundle of the ACL footprint. Thus, in comparison with cadaveric studies, transportal, and transtibial techniques are relatively higher.
With the modified transtibial technique, a deep and low femoral tunnel can be created, in contrast to the previous studies, which state that the transtibial technique tends to place the femoral tunnel shallow (anterior)[20] and high (roof of the notch).[21] This is, inturn, result of a medialised tibial tunnel, a tibial tunnel angulated towards posterior margin of ACL footprint near tibial plateau, an 11 mm tibial tunnel in addition to usage of posterior offset and a flexible reamer and guidewire. All these modifications collectively help us create a low and posterior femoral tunnel.
As the femoral tunnel position is dependent on the tibial tunnel in a transtibial technique, we have analyzed the tibial tunnel angulation and the intra-articular tibial aperture position to rule out any change that happens while trying to ream the femoral tunnel in the desired position.
The starting point of the guide pin on the tibial cortex for it to be centered on the femoral and tibial footprint was noted to be 13.7 mm from the tibial tubercle, 14.1 mm from the joint line, and have a coronal plane angulation of 42.1°, with respect to the knee in 90° flexion.[7] In our study, the starting point of the tibial guide pin was maintained medial to the usual entry point, such that the tibial tunnel drilled just encroaches the superficial MCL. This medialized tibial tunnel (compared to the normal tunnel position), along with the 11 mm wide tunnel diameter, allows us to adequately angulate and reach the posterior margin of the tibial footprint, close to the tibial plateau (unlike the usual center of the tibial footprint), thereby achieving a low and posterior position of the femoral tunnel.
Studies by Howell et al. on tibial tunnel suggest placement of the tibial tunnel mouth at the slope of the intercondylar roof, that is, 44% of the anteroposterior diameter of the joint line to avoid impingement.[22] Similarly, the intra-articular aperture of the tibia tunnel as measured by the reference method in our study, was noted as 41.89 ± 5.6% of the maximum anteroposterior diameter of the tibia. Although the measurement technique is different, the measurements were based on the anteroposterior diameter of the tibia.
The angle formed by the tibial tunnel in the coronal plane is the angle between the axis of the tibial tunnel and the line drawn along the tibial articular surface. Howell et al. stated that patients with this angle between 65 and 74° were found to have the least chance of loss of knee flexion and anterior laxity.[3] The tibial tunnel angle in the coronal plane in our study was 64.9 ± 3.5 degrees, which was comparable to Howell’s study. Heming et al. have stated in their study that in transtibial drilling, tunnels centralized over the ACL footprint can be produced in a bargain for the shorter tibial tunnel.[7]
In contrast to the standard transtibial technique, which carries the risk of a shorter tibial tunnel, by following the above-mentioned starting point, the tibial tunnel angle in the coronal plane and the intra-articular aperture position resulted in an ideal and desirable tibial tunnel. With this accuracy of the tibial tunnel and using the above-mentioned modified transtibial technique, an ideal femoral tunnel comparable to the one from the transportal technique or near-anatomical ACL (cadaver) can be obtained. Therefore, not only are the drawbacks of the transportal technique (graft passage difficulty and technical difficulties) avoided, but with the described technique, the risk associated with traditional transtibial techniques, such as high and shallow femoral tunnels and short tibial tunnels, is also eliminated. Unlike the earlier transtibial studies, we have examined the tibial tunnel position and angulation, which not only emphasizes the importance of the tibial tunnel in the transtibial technique but also standardizes it. The limitation of the study may be the usage of the mean value of femoral tunnel position from multiple previous studies for comparison. Although the method of comparison is similar in all the studies, individual values, standard deviation, size of the study population, and uniformity technique used were not clearly stated. There was no blinding done among the surgeon and radiologist who did the radiograph analysis of the study. For this modified transtibial technique to be reproducible, more randomized control studies involving larger study population sizes and longer follow-up periods are needed.
CONCLUSION
Therefore, our modified transtibial method of ACL restoration with BTB graft is not only a reproducible technique but also overcomes the drawback of the conventional transtibial method by making the femoral tunnel comparable to the femoral tunnel position acquired by the transportal technique and nearly anatomical compared to the native ACL.
Author contributions
HM: Data collection and manuscript writing; PJ: Manuscript editing and design of the research; VKG: Data acquisition and interpretation; SP: Critical analysis and review; AS: Conceptualization of the research and final approval; VM: Statistical analysis and data interpretation.
Ethical approval
This research/study was approved by the institutional ethics committee of Sri Ramachandra institute of higher education and research, CSP-MED/24/MAY/80/144,dated 06.05.24.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Autografts commonly used in anterior cruciate ligament reconstruction. J Am Acad Orthop Surg. 2011;19:259-64.
- [CrossRef] [PubMed] [Google Scholar]
- Transtibial versus anteromedial portal drilling for anterior cruciate ligament reconstruction: A cadaveric study of femoral tunnel length and obliquity. Arthroscopy. 2010;26:342-50.
- [CrossRef] [PubMed] [Google Scholar]
- The relationship between the angle of the tibial tunnel in the coronal plane and loss of flexion and anterior laxity after anterior cruciate ligament reconstruction. Am J Sports Med. 2001;29:567-74.
- [CrossRef] [PubMed] [Google Scholar]
- Knee stability and graft function after anterior cruciate ligament reconstruction: A comparison of a lateral and an anatomical femoral tunnel placement. Am J Sports Med. 2004;32:1825-32.
- [CrossRef] [PubMed] [Google Scholar]
- Vertical femoral tunnel placement results in rotational knee laxity after anterior cruciate ligament reconstruction. Arthroscopy. 2007;23:771-8.
- [CrossRef] [PubMed] [Google Scholar]
- Prevention of medial femoral condyle injury by using a slotted cannula in anterior cruciate ligament reconstruction. Arthrosc Tech. 2017;6:e1639-43.
- [CrossRef] [PubMed] [Google Scholar]
- Anatomical limitations of transtibial drilling in anterior cruciate ligament reconstruction. Am J Sports Med. 2007;35:1708-15.
- [CrossRef] [PubMed] [Google Scholar]
- Femoral insertion of the ACL. Radiographic quadrant method. Am J Knee Surg. 1997;10:14-21.
- [Google Scholar]
- Morphology of anterior cruciate ligament attachments for anatomic reconstruction: A cadaveric dissection and radiographic study. Arthroscopy. 2006;22:984-92.
- [CrossRef] [PubMed] [Google Scholar]
- Anatomical analysis of the anterior cruciate ligament femoral and tibial footprints. J Orthop Sci. 2008;13:122-9.
- [CrossRef] [PubMed] [Google Scholar]
- Anterior knee pain in ACL reconstruction with BPTB graft-is it a myth? Comparative outcome analysis with hamstring graft in 1,250 patients. J Orthop. 2020;22:408.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of femoral tunnel positioning using 3-dimensional computed tomography and radiographs after single bundle anterior cruciate ligament reconstruction with modified transtibial technique. Clin Orthop Surg. 2013;5:188-94.
- [CrossRef] [PubMed] [Google Scholar]
- Femoral footprint for anatomical single-bundle anterior cruciate ligament reconstruction: A cadaveric study. Knee Surg Relat Res. 2018;30:128.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of the quadrant method measuring four points and bernard method in femoral tunnel position evaluation on 3-dimensional reconstructed computed tomography after anatomical single-bundle anterior cruciate ligament reconstruction. BMC Musculoskelet Disord. 2024;25:558.
- [CrossRef] [PubMed] [Google Scholar]
- Factors affecting graft excursion patterns in endoscopic anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 1998;6(Suppl 1):S20-4.
- [CrossRef] [PubMed] [Google Scholar]
- Knee stability and graft function following anterior cruciate ligament reconstruction: Comparison between 11 o'clock and 10 o'clock femoral tunnel placement. Arthroscopy. 2003;19:297-304.
- [CrossRef] [PubMed] [Google Scholar]
- Increased risk of revision after anteromedial compared with transtibial drilling of the femoral tunnel during primary anterior cruciate ligament reconstruction: Results from the Danish Knee Ligament Reconstruction Register. Arthroscopy. 2013;29:98-105.
- [CrossRef] [PubMed] [Google Scholar]
- High non-anatomic tunnel position rates in ACL reconstruction failure using both transtibial and anteromedial tunnel drilling techniques. Arch Orthop Trauma Surg. 2017;137:1293-9.
- [CrossRef] [PubMed] [Google Scholar]
- Comparing the use of flexible and rigid reaming systems through an anteromedial portal for femoral tunnel creation during anterior cruciate ligament reconstruction: A systematic review. Orthop J Sports Med. 2021;9 Available from: http://dx.doi.org/10.1177/23259671211035741
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of transtibial and transportal techniques in drilling femoral tunnels during anterior cruciate ligament reconstruction using 3D-CAD models. Open Access J Sports Med. 2014;5:65.
- [CrossRef] [PubMed] [Google Scholar]
- Transtibial versus anteromedial portal of the femoral tunnel in ACL reconstruction: A cadaveric study. Knee. 2008;15:364-7.
- [CrossRef] [PubMed] [Google Scholar]
- Failure of reconstruction of the anterior cruciate ligament due to impingement by the intercondylar roof. J Bone Joint Surg Am. 1993;75:1044-55.
- [CrossRef] [PubMed] [Google Scholar]




