
Translate this page into:
History of foot and ankle arthroscopy

-
Received: ,
Accepted: ,
How to cite this article: Dhillon MS, Hooda A, Kumar P. History of foot and ankle arthroscopy. J Arthrosc Surg Sport Med 2020;1(1):126-132.
Abstract
Historically, arthroscopy originated from the concept of cystoscopy, and was limited to use in the large joints, principally the knee. It is only the past 50 years that has led to the techniques being applied to the small joints of the foot and ankle, and the success has mirrored the development of better lens systems and smaller instruments. Although Watanabe pioneered arthroscopy as a whole, and initiated foot-and-ankle arthroscopy, it was the fine tuning of techniques for the ankle and subtalar joints by pioneers such as Van Dijk in Europe and Ferkel in USA, who combined their innovative techniques along with extensive teaching worldwide that lead to its acceptance in the current form. Although limited in scale, arthroscopy of the foot and ankle is currently practiced in many centers in India, with trained surgeons applying latest techniques at a few centers. The current status of arthroscopy is that it has allowed minimally invasive surgery in smaller and smaller joints, with a huge potential for expansion in the future.
Keywords
Ankle
Arthroscopy
Foot
History
Subtalar joint

INTRODUCTION
The evolution of arthroscopic surgery has been one of the most significant advances in orthopedics.[1] It has revolutionized interventions in the form that by minimally invasive methods the surgeon is able to visualize areas of the joint or even the bone which previously accessible only by large incisions.
Historically arthroscopy has evolved along with the evolution of optical instruments, specific punches and grabbers, as well as motorized equipment. This has allowed the application of arthroscopy into smaller and smaller joints, which has in turn benefited the foot-and-ankle region. The biggest joints of the body have always taken precedence and have been the sites of most major developments, as was the case with the development of arthroscopy. Most of the focus at the origin of arthroscopy was at the knee or the hip, principally because these are large joints and the pathology and disability associated with these are significant. Over the ages, the foot as an area of specialized care has been considered somewhat less important: If you look at the evolution of arthroscopy of the foot and ankle, the same is reflected in its history.[2]
Technically speaking, the ankle joint, the subtalar joint, and the small joints of the foot have been considered tight joints, with planar surfaces and limited mobility, which led to them being considered relatively unfit for arthroscopic evaluation. It was the evolution of thinner telescopes and better optics along, with smaller instrumentation and aids to distract joint, that arthroscopic interventions for these joints evolved.[3]
It is fairly easy to trace the history of the development of foot and ankle arthroscopy; being a recent advance dating <100 years, the documentation associated with arthroscopy is easy to access and the historical changes can be easily listed in chronological order.[4,5] The current article tries to document this evolution in the foot and ankle from a historical perspective, and tries to identify the key players who have made foot-and-ankle arthroscopy the success it is today in modern orthopedics.
TIME FROM CYSTOSCOPY TO ARTHROSCOPY- INCEPTION INTO ORTHOPEDICS
In the 18th-century, endoscopes were used to examine ears, nose, and vagina using natural light.[6] Cystoscopes were developed in the 19th century, which used mirrors and light from combustion to see into the urinary bladder.[7] The term arthroscopy was first used by a Danish surgeon/ radiologist, Severin Nordentoft, who presented a paper at the 41st congress of the German Society of Surgery at Berlin in 1912; he used an endoscope similar to the thoracoscope to diagnose a meniscal tear of the knee.[8] Subsequently, in 1918 a Japanese surgeon, Kenji Takagi, tried this technique on a cadaveric knee using a cystoscope, but failed due to limitations of the instrument. He went on to devise a 7.3 mm arthroscope without a lens and performed his first successful arthroscopy on a difficult tubercular knee.[9] Both Takagi and Nordentoft are recognized as the early pioneers of this minimally invasive surgery, which now is universally called arthroscopy.[10] Their attempts were primarily diagnostic, not therapeutic, which seems to be in tune with the equipment available at that time. In 1921, Eugen Bircher in Switzerland published his extensive work on arthroscopy and practiced it in Europe. He used a modified Jacobaeus laparoscope to visualize the interior of the knee in 18 patients in Switzerland and later published his findings on post-traumatic arthritis and the diagnosis of meniscal pathology. Later, he became frustrated due to the limitation of instruments and gave up arthroscopy in 1930.[11] Unfortunately in that historical period, the sharing of scientific work and the evolution of medicine were developed only in three large blocks; Europe, United States of America, and Japan, all of whom worked independently at that time. Most publications were made in the native languages, with no exchange of new research and ideas, limiting the scope of such techniques.[12]
Bircher’s work was largely neglected until re-evaluated by Masaki Watanabe in 1975.[13] By this time in history, there was a significant evolution of arthroscopic instruments; aids such as trocar tip, development of thinner arthroscopes, and cameras with color contrast and better lens systems, along with better techniques of aiding joint visualization such as pressure pumps and distractors led to the birth of Modern Arthroscopy. By 1954 a direct viewing arthroscope had been designed, having a telescope of 5 mm inserted through a 6 mm outer sheath. It was suitable for diagnostic purposes; gradually with several trials and errors, Watanabe designed what he called the “no. 21 arthroscope” in 1958. This was later used in 1962, for the first-ever case of arthroscopic meniscectomy in a boy who had suffered a knee injury while playing basketball; the patient had a flap tear of the medial meniscus and was discharged on the same day.[14] He subsequently returned to basketball after 6 weeks. Watanabe described the years 1970–1978 as the “third stage of the evolution of arthroscopy,” wherein feasibility of scopes for smaller and tighter joints was explored, which grew with the development of the Selfoc arthroscope in 1970; subsequently after improvements this came to be known as the “selfoscope.”[14] He was able to perform ankle arthroscopy and described related portals for the same in 1972, a decade later than his first successful therapeutic knee arthroscopy. This subsequently led to the foundation of arthroscopy in both therapeutic and diagnostic fields.
FROM LARGE TO SMALLER JOINTS – THE EVOLUTION TO ANKLE/FOOT ARTHROSCOPY
Foot and ankle arthroscopy in its modern form has evolved at a relatively slower pace over the years. As compared to other larger joints such as the knee and shoulder, its application is significantly less, with the foot/ankle arthroscopies being performed at fewer centers. The arthroscopy of the smaller joints started late, and evolved later, and that too with the advent of smaller, more appropriate instruments and scopes. In 1968, the Nippon Sheet glass company in Japan developed a 1mm lens called Selfoc.[13] Watanabe [Figure 1] was aware of the development and proposed its usage for the study of smaller joints. In 1970, a smaller arthroscope with 1.7 mm apical diameter and a 2 mm base for the portal was ready, which allowed accessing the smaller joints of the body, which were previously not considered amenable to arthroscopic techniques. The brightness and clarity were later modified by Olympus optical company and led to the development of a smaller arthroscope to study small joints such as elbow and ankle.[13,14]

- Masaki Watanabe considered to be the father of arthroscopy (source :https://images.app.goo.gl/cDXsFGkBTmW8KZL8A).
To chronicle the of evolution in the history of modern orthopedics, the authors did a PubMed search with keywords – ((“ankle”[MeSH Terms] OR “ankle”[All Fields] OR “ankle joint”[MeSH Terms] OR (“ankle”[All Fields] AND “joint”[All Fields]) OR “ankle joint”[All Fields]) AND (“foot”[MeSH Terms] OR “foot”[All Fields]) AND (“arthroscopy”[MeSH Terms] OR “arthroscopy”[All Fields])), which yielded a total of only 1057 hits. On evaluating the number of hits, the data reflect that the pace of evolution has been slow but is multiplying rapidly; between 1981 and 1990, there are only 25 hits, which increased to 74 between 1991 and 2000 (a 3 fold increase), further increasing to 249 hits between 2001 and 2010 (another 3 fold increase) and the past 10 years have seen another three-fold surge, 743 hits from 2011 to 2020.
A similar PubMed search over the same time period using keywords – (“knee”[MeSH Terms] OR “knee”[All Fields] OR “knee joint”[MeSH Terms] OR (“knee”[All Fields] AND “joint”[All Fields]) OR “knee joint”[All Fields]) AND (“arthroscopy”[MeSH Terms] OR “arthroscopy”[All Fields]) yielded a total of 14433 hits. On evaluating further, the number of hits increased over time, from 1981 to 1990 showed 1335 hits, which doubled in the next 10 years, i.e. 2624 from 1999 to 2000, gradually rose to 4382 between 2001 and 2010 and 6013 in past 10 years. This data reveal that there has been a steady rise in the number of related hits with time as far as the knee joint is concerned which was, and still is, the most common joint that is scoped all around the world.
When we compare the number of hits in the last decade with that for the knee joint itself, there is 66% rise of publications focused on foot-and-ankle arthroscopy compared to a 27% rise in publications focused on knee arthroscopy [Graphs 1 and 2]. This further signifies the late, but subsequently significant interest and expansion of arthroscopy from the large to smaller joints.
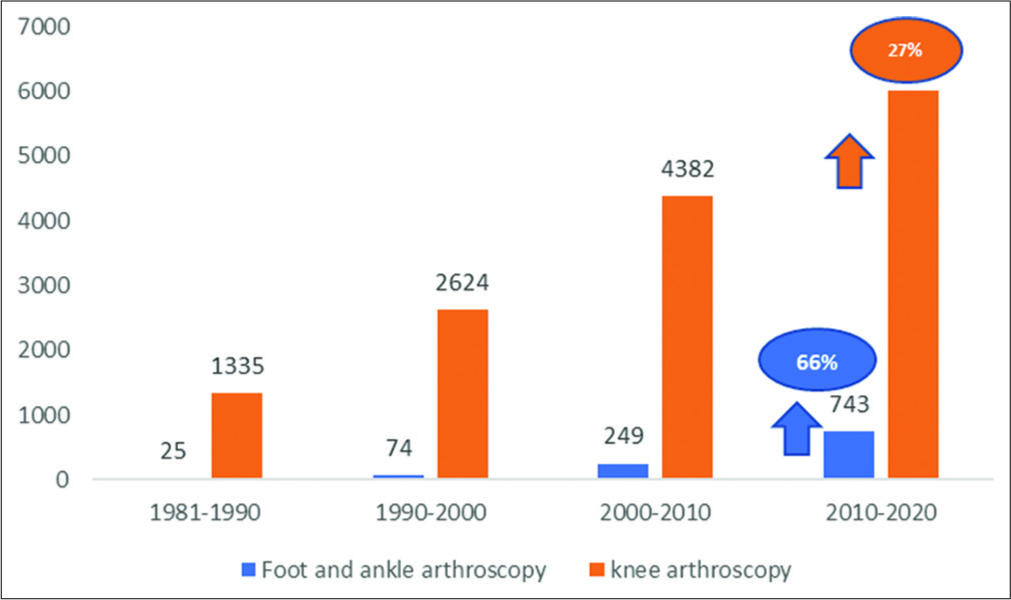
- Comparison of the number of hits on PubMed in last four decades with keywords – foot-and-ankle arthroscopy and knee arthroscopy.

- Comparison of publication trends for knee, ankle, and subtalar arthroscopy.
ANKLE ARTHROSCOPY
Ankle arthroscopy was regarded as a great addition to the armamentarium of the foot-and-ankle surgeons. It permitted the direct visualization of intra-articular pathology, and arthroscopically performed surgical procedures in the ankle were generally linked to faster rehabilitation, lesser morbidity, and better cosmetic results when compared to conventional open surgeries.[15] A 30° 4.0-mm arthroscope or an oblique 70° arthroscope or a short 2.7-mm, wide- angle 30° arthroscope may be used in ankle arthroscopy. Ankle arthroscopy can now be categorized into anterior and posterior ankle arthroscopy, with the ability to visualize different compartments of the joint providing opportunities for therapy beyond its diagnostic role. This has also developed historically in the past 30 years only.
As far back as 1939, Takagi, the pioneer of arthroscopy, when publishing his experience, included one arthroscopy of a flail ankle.[9,16] In the 1930s, Burman was the first to attempt ankle arthroscopy in the United States at the hospital for joint diseases in New York, and also published the difficulties related to ankle arthroscopy with larger instruments.[17] Watanabe developed a fiberoptic arthroscope in 1970, and also published a report on 28 ankle arthroscopies in 1972, where he described the standard anterolateral, anteromedial, and posterior portals to the ankle joint.[18] The surgical anatomy description was significantly refined by Chen et al. in 1976 after they published a series of 67 ankle arthroscopies in which he described compartments within the ankle joint and their surgical anatomy.[19]
In the past two decades, many authors have published their work on ankle arthroscopy, outlining their experience and surgical techniques.[20-22] Historically, the indications for ankle arthroscopy fall into two broad categories, i.e., diagnostic and therapeutic. An undiagnosed ankle pain, persistent unexplained swelling, locking suggestive of loose bodies, or nonspecific synovitis historically came under diagnostic indications.[23] Therapeutic indications have involved significantly, and now include treatment of stiff ankle more commonly – arthrofibrosis after fracture,[24] removal of soft-tissue impingement or loose bodies[25] and treatment of osteochondral lesions of the talar dome.[26,27] The treatment of infective arthritis has also been assisted by ankle arthroscopy.[28,29] These indications have now actually fused together in the 21st century, and there is rarely a case where a diagnostic arthroscopy is not immediately combined with a therapeutic procedure. Finesse in ankle arthroscopy was largely achieved by the addition of multiple posterior portals and aids in distracting the joints.[30] Van Dijk [Figure 2] from Holland has been one of the big pioneers, and now the combined use of anterior and posterior portals is common place.[31] Richard Ferkel [Figure 3] established the specialty in the USA, and demonstrated to wide audiences his methods of arthroscopic evaluation of all foot joints, including the small joints of the toe. Talar osteochondral lesions are now managed purely arthroscopically, which could be a combination of anterior or posterior portals, or even transmalleolar.[26]

- Niek van Dijk of Netherlands, a pioneer of ankle and subtalar arthroscopy in Europe, seen here with the author.

- Richard Ferkel of USA, who pioneered ankle and subtalar arthroscopy in the USA (Source: https://images.app.goo.gl/5grFAnyMjU2cUz7RA).
Today, arthroscopy of the ankle is routinely used to assist the reduction of major articular fractures, with “dry arthroscopy” assisting reduction of pilon and talus fractures.[32]
Syndesmosis evaluation and treatment using arthroscopy as a visual, minimally invasive aid was propagated by Lee et al.;[33] even lateral ankle ligament injuries are being addressed with the help of arthroscopes.[34] Ankle fusion is another area where the arthroscope has become a significant aid. Morgan first described the arthrodesis of the tibiotalar joint with the help of arthroscopy and called it as an arthroscopy assisted ankle arthrodesis.[23] At present, most trained surgeons are using this as the method of choice, unless there are specific contraindications like significant deformity that needs to be corrected at the same time.
SUBTALAR ARTHROSCOPY
The complex anatomy of the subtalar joint has historically made its arthroscopic evaluation difficult; however, the evolution of instruments and distraction methods has made subtalar arthroscopy increasingly feasible.
Subtalar arthroscopy was first described by the Parisien et al. in 1986 in which he assessed the articular cartilage in cases of arthritis and also evaluated the cause of chronic pain syndrome.[35] Marumoto and Ferkel in 1991, described the use of a posterolateral portal in addition to standard anterior arthroscopy, through which they addressed os trigonum or posterior osteochondral lesions.[36] Even today, subtalar arthroscopy is mainly diagnostic, and only the posterior facet is visualized. The 1.9-mm or the 2.7-mm 30° short wide-angle arthroscopes are the ones most frequently used.
A PubMed search with keywords – (“subtalar joint”[MeSH Terms] OR (“subtalar”[All Fields] AND “joint”[All Fields]) OR “subtalar joint”[All Fields]) AND (“arthroscopy”[MeSH Terms] OR “arthroscopy”[All Fields]) showed 195 hits. On detailed evaluation it showed only five hits from 1981 to 1990, increased to 21 in 1991–2000, followed by a three- fold rise with 72 hits between 2001 and 2010 and gradually increased to 99 in the past 10 years.
Varying techniques of hindfoot arthroscopy to treat both soft-tissue and osseous lesions have been described. Van Dijk et al.[31] were the first to describe a technique allowing 2-portal access to the hindfoot, including the posterior ankle and subtalar joints, which gave access to both intra- and extra-articular structures of the hindfoot, including the flexor hallucis longus tendon and os trigonum.
Parisien et al. suggested and described arthroscopic subtalar arthrodesis (ASA), which as an orthopedic intervention has evolved from the 1990s. A PubMed search with keywords: Arthroscopic [All Fields] AND (“ankle”[MeSH Terms] OR “ankle”[All Fields] OR “ankle joint”[MeSH Terms] OR (“ankle”[All Fields] AND “joint”[All Fields]) OR “ankle joint”[All Fields]) AND (“arthrodesis”[MeSH Terms] OR “arthrodesis”[All Fields]), yield 0 hit in 1980’s. Between the years 1991 and 2000, there were 35 hits; 2001–2010: 49 hits and 138 hits after 2011. ASA is now recommended over open procedures for its therapeutic benefits in decreasing infection and nonunion rates.[31,37,38] With access to subtalar and talonavicular joints possible, the applications and scope of arthroscopy in this area have widened. Arthroscopic management of post-traumatic hindfoot stiffness due to capsular fibrosis, tendon adhesions and even calcaneal malunions leading to decrease inversion, has been described by Lui et al.[37] Interchangeable portals such as medial and dorsomedial midtarsal portal provide reasonable access to the talonavicular joint; medial midtarsal and medial tarsal canal portals are useful for medial subtalar arthroscopy for stiffness cases [Figure 4].[37]
SMALL TO SMALLER-FIRST METATASOPHALANGEAL JOINT ARTHROSCOPY
Among other things relating to arthroscopy, Watanabe was the first to describe the arthroscopy of the first metatarsophalangeal joint in 1971.[13] The indications were almost similar to subtalar arthroscopy but small instruments were essential such as 1.9 mm or 2.7 mm arthroscope with small radius resectors.
Ferkel and Van Buechen[39] published a series of the first metatarsophalangeal joint debridements with 83% good or excellent clinical results in April 1991. In 2009, Siclari et al. described arthroscopic lateral release and percutaneous distal osteotomy for hallux valus.[40] Recently, Lui also describe the technique of arthroscopic assisted arthrodesis in fixed hallux varus.[41]
TENDOSCOPY
The word tendoscopy literally means endoscopy of the tendon sheath and was first proposed by Wertheimer in 1995.[42] It is one of the latest additions in arthroscopy; where a 2.7 mm 30 degrees arthroscope is inserted anywhere along the length of the tendon.
In 1997, Van Dijk et al. gave the first description of different tendoscopic techniques for both diagnosis and treatment in a variety of tendinopathies, first on cadaver and later on nine patients.[43] It is chiefly used as a primary procedure or as an adjuvant with open surgery. The main indications are tenosynovitis, degenerative tendinopathy or dislocations of peroneal tendons, tibialis posterior, and Achilles tendon more commonly.[44,45]
FOOT-AND-ANKLE ARTHROSCOPY IN INDIA
Looking at the Indian perspective, foot/ankle arthroscopy is still in its infancy; although knee arthroscopy took off in the early 1980s, with most centers in India doing this as a routine, foot/ ankle arthroscopy is still limited to a few centers, and that too in the major cities.[5] The principal author learned the science and skills of ankle arthroscopy from Nicholas Antao of Mumbai, who was perhaps the first surgeon in India to practice this in the 1980s. The premier institutes of the nation are teaching and propagating this in 2020, as are a few dedicated foot and ankle surgeons. Nevertheless, a lot more has be done before foot and ankle arthroscopy becomes common place. A chronicler of history and development of this particular procedure 20 years from today may have a different tale to tell.
CONCLUSION
Historically speaking, foot and ankle arthroscopy has lagged behind in its development; the pioneers of arthroscopy in the foot and ankle like van Dijk and Ferkel carried forward the work of Watanabe and Tagaki in Japan, and took this specialized field beyond the frontiers defined by surgeons of the mid-1990s. They were aided by development of smaller arthroscopes, smaller instruments, and better distraction methods. In the third decade of the 21st century, we now stand at the threshold of increasing accessibility of even the smaller joints of foot and ankle, which has allowed faster rehabilitation, better cosmesis, and outcomes.

- Time line describing the evolution of foot and ankle arthroscopy.
Declaration of patient consent
Patient’s consent not required as there are no patients in this study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- History arthroscopic surgery In: Shahriaree H, ed. O'Connor's Textbook of Arthroscopic Surgery (1st ed). Philadelphia, PA: JB Lippincott; 1983.
- [Google Scholar]
- Evolution and current status of arthroscopic surgery in India. J Postgrad Med Educ Res. 2018;52:22-5.
- [CrossRef] [Google Scholar]
- Two centuries of cystoscopy: The development of imaging, instru-mentation and synergistic technologies. BJU Int. 2008;103:154-8.
- [CrossRef] [PubMed] [Google Scholar]
- Eugen Bircher (1882-1956) the first knee surgeon to use diagnostic arthroscopy. Arthroscopy. 2003;19:771-6.
- [CrossRef] [Google Scholar]
- Selfoc-Arthroscope (Watanabe No. 24 Arthroscope) Monograph Tokyo: Tushin Hospital; 1972.
- [Google Scholar]
- Arthroscopy of direct visualization of joints: An experimental cadaver study. J Bone Joint Surg. 1931;13:669.
- [Google Scholar]
- Clinical and cadaver studies on the ankle joint arthroscopy. J Jpn Orthop Assoc. 1976;50:631.
- [Google Scholar]
- Arthroscopic treatment of ankle injuries (review) Othop Clin North Am. 1994;25:17-32.
- [Google Scholar]
- Arthroscopy of the ankle: Technique and normal anatomy. Foot Ankle. 1985;6:29e33.
- [CrossRef] [PubMed] [Google Scholar]
- Ankle arthroscopy: Review and long term results. Foot Ankle. 1992;13:382-5.
- [CrossRef] [PubMed] [Google Scholar]
- Arthroscopic treatment of anterolateral impingement of the ankle. Am J Sports Med. 1991;19:440-6.
- [CrossRef] [PubMed] [Google Scholar]
- Arthroscopic treatment of osteochondral lesions of the talus: Technique and results. Orthop Trans. 1990;14:172-3.
- [Google Scholar]
- Arthroscopic drilling with debridement of remaining cartilage for osteochondral lesions of the talar dome in unstable ankles. Am J Sports Med. 2004;32:332e6.
- [CrossRef] [PubMed] [Google Scholar]
- Anatomic study of the arthroscopic debridement of the ankle. Foot Ankle Int. 1994;15:614-21.
- [CrossRef] [PubMed] [Google Scholar]
- Arthroscopic tibiotalar arthrodesis In: McGinty JB, Jackson RW, Poehling GG, Caspari RB, eds. Operative Arthroscopy. New York: Raven Press; 1991. p. :695701.
- [Google Scholar]
- New concepts (distraction) in ankle arthroscopy. Arthroscopy. 1998;4:160-7.
- [CrossRef] [Google Scholar]
- A 2-portal endoscopic approach for diagnosis and treatment of posterior ankle pathology. Arthroscopy. 2000;16:871-6.
- [CrossRef] [PubMed] [Google Scholar]
- Arthroscopic syndesmotic repair: Technical tip. Foot Ankle Int. 2015;36:229-31.
- [CrossRef] [PubMed] [Google Scholar]
- Arthroscopic lateral ankle ligament reconstruction. Tech Foot Ankle Surg. 2011;10:111-6.
- [CrossRef] [Google Scholar]
- Arthroscopy of the posterior subtalar joint: A preliminary report. Foot Ankle. 1986;6:219-24.
- [CrossRef] [PubMed] [Google Scholar]
- Arthroscopic excision of the os trigonum: A new technique with preliminary clinical results. Foot Ankle Int. 1997;18:777-84.
- [CrossRef] [PubMed] [Google Scholar]
- Arthroscopic and endoscopic management of posttraumatic hindfoot stiffness. Indian J Orthop. 2018;52:304-8.
- [CrossRef] [PubMed] [Google Scholar]
- Arthroscopy of the subtalar joint: An experimental approach. Arthroscopy. 1985;1:53-7.
- [CrossRef] [Google Scholar]
- Great toe Arthroscopy: Indications, Technique, and Results San Diego: The Arthroscopy Association of North America's Annual Meeting; 1991.
- [Google Scholar]
- Arthroscopic lateral release and percutaneous distal osteotomy for hallux valgus: A preliminary report. Foot Ankle Int. 2009;30:675-9.
- [CrossRef] [PubMed] [Google Scholar]
- Arthroscopic first metatarsophalangeal arthrodesis for repair of fixed hallux varus deformity. Foot Ankle Surg. 2015;54:1127-31.
- [CrossRef] [PubMed] [Google Scholar]
- The role of endoscopy in treatment of stenosing posterior tibial tenosynovitis. J Foot Ankle Surg. 1995;34:15-22.
- [CrossRef] [Google Scholar]
- Tendoscopy in stage 1 posterior tibial tendon dysfunction. Foot Ankle Clin. 2012;17:399-406.
- [CrossRef] [PubMed] [Google Scholar]
- Endoscopic surgery in chronic Achilles tendinopathies: A preliminary report. Arthroscopy. 2002;18:298e303.
- [CrossRef] [PubMed] [Google Scholar]




