
Translate this page into:
Pes planus intermetatarsal angle to measure flatfoot deformity on dorsoplantar radiographic imaging
*Corresponding author: Rajesh Botchu, Department of Musculoskeletal Radiology, Royal Orthopedic Hospital, Birmingham, United Kingdom drrajeshb@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Giliyaru S, Gavvala SN, Saad A, Jenko N, Iyengar K, Nischal N, et al. Pes planus intermetatarsal angle to measure flatfoot deformity on dorsoplantar radiographic imaging. J Arthrosc Surg Sports Med. 2024;5:71-4. doi: 10.25259/JASSM_17_2024
Abstract
Objectives:
Pes planus, or “flat foot,” is a common foot condition involving talus misalignment, calcaneus eversion, medial arch collapse, and forefoot abduction. It is a well-recognized cause of foot pain and can lead to disability in patients. Clinical diagnosis is supported by plain radiography. However, in patients presenting with foot pain, traditionally dorsoplantar (DP) and oblique radiographs are undertaken. Pes planus may be difficult to analyze and classify on predominant DP and oblique radiographs and often requires weight-bearing lateral foot radiographs to direct patient management. Our study introduces a novel angle for pes planus diagnosis on DP radiographs of the foot. The purpose of this study was to describe a new radiological pes planus intermetatarsal angle (PPIMA) for assessment of flatfoot DP imaging of the foot.
Materials and Methods:
We performed a retrospective cohort study on 114 consecutive patients presenting with foot pain referred to our foot and ankle clinic weight-bearing DP, oblique radiographs of the foot and lateral radiographs of the foot and ankle were undertaken. Demographic details and clinical indication were recorded, and radiological parameters of hallux valgus angle, calcaneal pitch and angle between the shaft of the first and fifth metatarsal PPIMA were measured by two consultant radiologists and a radiology trainee. Data were organized using Microsoft Excel, and statistical analysis was performed STATA (StataCorp LLC, College Station, TX, USA) using analysis of variance and post hoc analysis.
Results:
Thirty patients were excluded due to the presence of hallux valgus deformity. In our study, the cohort with normal foot alignment (n = 30, age 14–18) had an average PPIMA of 20.7°, pes cavus (n = 3, age 14–18) average PPIMA was 24.0, while the pes planus group (n = 51, age 14–18) had an average PPIMA of 20.0°. There was no statistically significant difference in PPIMA between the groups (P = 0.229).
Conclusion:
Our study introduces a practical diagnostic tool for pes planus on DP foot imaging. The PPIMA is not a reliable indicator for the evaluation of foot alignment.
Keywords
Adult-acquired flatfoot deformity
Pes planus
Hallux valgus angle
Intermetatarsal angle
Radiography

INTRODUCTION
Pes planus, also known as “flat foot,” is a common podiatric condition characterized by a malalignment of the foot, including medial rotation and plantar flexion of the talus, eversion of the calcaneus, collapse of the medial arch, and forefoot abduction.[1] This condition often brings the region of the foot closer to the ground or in contact with the ground surface. The medial longitudinal arch of the foot plays a pivotal role in supporting the body, absorbing the forces during weight-bearing, and storing energy throughout the gait cycle.[2] While arch dysfunction is typically asymptomatic, some studies have linked flat feet to pain, instability, uneven distribution of plantar pressure, gait abnormalities, and foot fatigue.[3,4] These issues can significantly affect daily activities.[5]
Pes planus can be a congenital or acquired condition.[1,6,7] Acquired pes planus is often associated with posterior tibial tendon dysfunction and can be triggered by midfoot or hindfoot injuries. Soft-tissue injuries, such as those affecting the plantar fascia or spring ligament, are other common causes.[1,7,8-11]
Diagnosing pes planus can be relatively straightforward and often involves weight-bearing lateral foot radiographs. For instance, talo-first metatarsal and calcaneal inclination angles, measured on weight bearing lateral ankle view (WBLA), can diagnose pes planus.[1] Nonetheless, in our foot and ankle clinic, many patients with foot pain receive only dorsoplantar (DP) and oblique radiographs rather than a WBLA radiograph. Given that pes planus is a common source of foot pain, this may be missed on the DP radiographs. We hypothesis that the angle between the first and fifth metatarsal on DP radiograph can help to assess for pes planus. This approach allows us to triage patients with foot pain caused by pes planus efficiently.
MATERIALS AND METHODS
The Local Ethical Committee approval was obtained for this study. In this retrospective study, we reviewed the records of 114 consecutive patients who presented at our foot and ankle clinic with complaints of “foot pain.” Our dataset included patient demographics and relevant diagnostic imaging, including DP, oblique, and WBLA X-rays. We excluded patients with pre-existing foot deformities, hallux valgus, active infections, tumors, or a history of prior foot and ankle surgeries. We excluded hallux valgus as the first metatarsal is adducted, and this might alter the pes planus intermetatarsal angle (PPIMA). First metatarsophalangeal angle less or equal to 15° is considered as normal and over 15° is hallux valgus. Thirty cases were excluded due to the presence of hallux valgus.
We calculated the first metatarsophalangeal angle and calcaneal pitch for each patient, utilizing these measurements to identify 30 patients with normal foot and ankle radiographs (without pes planus), 3 with pes cavus and 51 patients with pes planus. Calcaneal pitch between 20° and 30° is considered as normal, <20° is pes planus and more than 30° as pes cavus.
The study’s primary purpose was to introduce a novel parameter, the PPIMA. The PPIMA involves measuring an angle formed by drawing a line from the first metatarsal to a second line originating from the fifth metatarsal on DP radiographs. A line is drawn along the midshaft of the first and fifth metatarsals by joining the midpoint of the proximal and distal shafts of the metatarsals. The angle between these two lines is PPIMA [Figures 1 and 2]. The first metatarsophalangeal angle is calculated by measuring the angle between the lines drawn along the shaft of the first metatarsal and the proximal phalanx of the big toe. Calcaneal pitch is calculated between the horizontal and line drawn along the inferior part of the calcaneum. The measurements were performed by a consultant radiologist and radiology trainee.
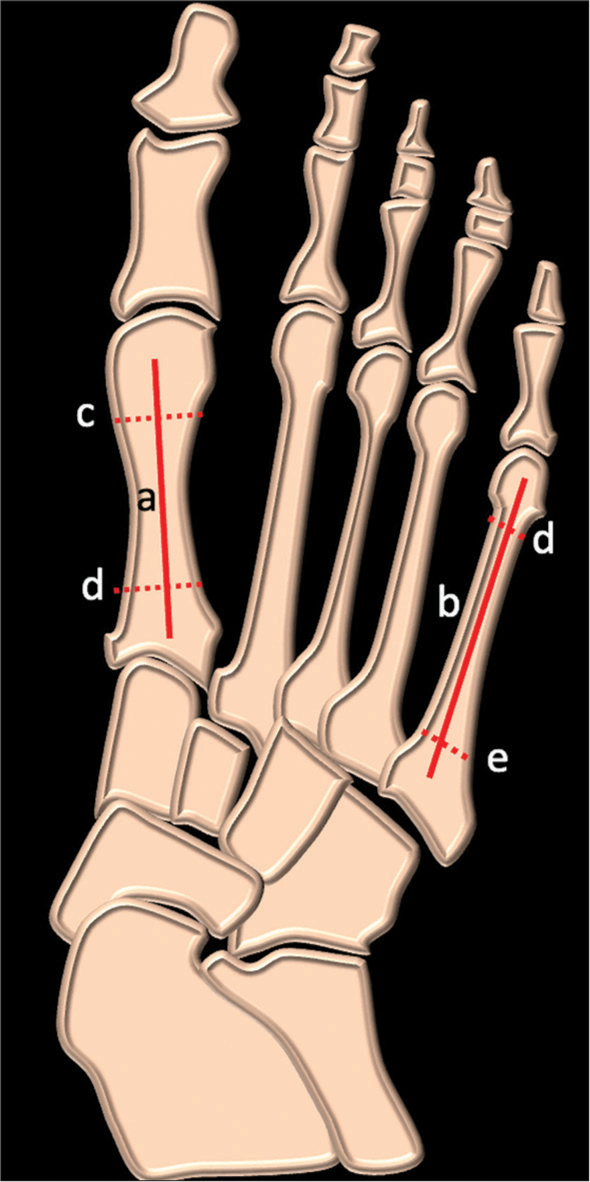
- Schematic of dorsoplantar radiographs of foot showing angle between line a (along the shaft of first metatarsal) and line b (line along the shaft of fifth metatarsal), this is drawn by joining the midpoints of the proximal and distal shaft of metatarsal (dotted lines c, d, e)

- Dorsoplantar radiograph of the foot showing the angle between the lines (yellow) along the shaft of the first and fifth metatarsals.
Data were recorded and organized using Microsoft Excel, and later, statistical analysis was conducted using STATA using analysis of variance (ANOVA) and pair-wise comparison with Sidak’s correction. P < 0.05 was considered to be significant. An intraclass correlation test was performed for inter- and intraobserver reliability.
RESULTS
Within our study, three cohorts were selected after excluding patients with hallux valgus deformity. In a cohort of 30 patients with normal foot alignment, there were 18 males and 12 females, with an average age of 16.3 years (standard deviation (SD) 1.29). This group’s average PPIMA measurement was 20.7 (SD 3.89, range 12–27°). In the second cohort of 50 patients with pes planus based on calcaneal pitch, there were 30 males and 20 females, with a mean age of 15.61 (SD 1.23). The mean PPIMA for these patients was 20.0° (SD 4.82, range 11–34). There were three patients with pes cavus, two males and one female, with an average age of 15.0 (SD 1.0) years. PPIMA of the pes cavus cohort was 24° (SD 1.0, range 22–26). Statistical analysis using ANOVA for all three groups (pes planus, pes cavus, and normal) showed no significant difference, with P-value of 0.229. Post hoc analysis using Sidak’s correction demonstrated no statistically significant difference between normal and pes planus groups (P = 0.890) [Table 1]. There was good intra- and interobserver reliability with a kappa of 0.8.
| Normal Patients | Pes Planus Patients | Pes Cavus Patients | |
|---|---|---|---|
| Average Age | 16.3 | 15.6 | 15.0 |
| Maximum Age | 18 | 18 | 16 |
| Minimum Age | 14 | 14 | 14 |
| Female | 12 | 20 | 1 |
| Male | 18 | 30 | 2 |
| Intermetatarsal Angle | |||
| Average | 20.7 | 20.0 | 24.0 |
| Standard Deviation | 3.89 | 4.82 | 1.0 |
DISCUSSION
Pes planus, commonly known as flat foot, is not an uncommon source of foot discomfort, with its prevalence varying across age groups, populations, and comorbidities.[12] This condition’s pathophysiology involves a biomechanical disorder affecting the alignment of the anterior transverse arch and the two longitudinal arches (medial and lateral), mainly focusing on the essential bones constituting the medial longitudinal arch.[3] Maintaining the structural integrity of this arch involves a complex interplay of structures such as the plantar fascia, plantar ligaments, and dynamic support from the posterior tibialis tendons and long peroneal muscles, often referred to as intrinsic foot muscles.[3] Dysfunction in any of these components can lead to a flattened medial longitudinal arch, resulting in an uneven weight distribution and the potential development of degenerative and painful conditions.[1-5]
The exact cause of primary symptomatic flatfoot is still unknown. Yet, it is associated with the repetitive overloading of the medial column, leading to the weakening or dysfunction of ligaments and tendons that stabilize the medial column.[3,13,14] This manifests as clinical and radiographic bony deformities characteristic of affected individuals.[15-17] Foot pain in flatfoot patients can be attributed to several factors, including excessive pronation, reduced shock absorption compared to normal feet, and increased stress on various foot structures.[1,14,15] The tibialis posterior muscle, a dynamic supporter of the medial arch, plays a critical role in controlling pronation and supination during the gait cycle.[18-21] Dysfunction of this muscle is a common issue in individuals with flat feet. It is important to note that radiographic deformity severity does not always correlate with symptoms, and the onset of flatfoot deformity can be insidious. Early recognition of radiographic signs is crucial.[20,21]
The lateral subluxation of the navicular on the talus (indicating talonavicular uncoverage and forefoot abduction) is valuable for pes planus evaluation on anteroposterior views.[22] However, this measurement typically becomes prominent in more advanced stages of pes planus and can undoubtedly be challenging to measure by more junior clinicians adequately. Other well-established measurements are the talar-first metatarsal angle and calcaneal pitch,[3] offering a more direct assessment of pes planus. However, these angles are observed on weight-bearing lateral views, often not obtained in patients with foot pain.
Our study introduces a novel and simple diagnostic angle; however, this was not shown to discriminate between normal, pes planus, and pes cavus. With minimal complexity, this measurement’s ease of application on DP radiographs ensures high reproducibility.
Limitations
Our study has a few limitations. First, this was a retrospective study. Second, clinical correlation was not performed. We excluded hallux valgus as in our experience that there is adduction of first metatarsal and this might alter the PPIMA.
CONCLUSION
PPIMA cannot reliably assess for foot alignment (normal pes planus and pes cavus) on DP radiographs.
Ethical approval
The Institutional Review Board approval is not required since it was a retrospective study.
Declaration of patient consent
Patient’s consent was not required as there are no patients in this study.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Pes cavus and pes planus. Analyses and treatment. Phys Ther. 1987;67:688-94.
- [CrossRef] [PubMed] [Google Scholar]
- Flatfoot and normal foot a comparative analysis of the stress shielding. J Orthop. 2018;15:820-5. Erratum in: J Orthop 2020;24:293
- [CrossRef] [PubMed] [Google Scholar]
- Pes planus: A review of etiology, diagnosis and chiropractic management. J Manipulative Physiol Ther. 1983;6:185-8.
- [Google Scholar]
- Pediatric flexible flatfoot; clinical aspects and algorithmic approach. Iran J Pediatr. 2013;23:247-60.
- [Google Scholar]
- Posterior tibial tendon dysfunction: An overlooked cause of foot deformity. J Family Med Prim Care. 2015;4:26-9.
- [CrossRef] [PubMed] [Google Scholar]
- Unusual variant of the nutcracker fracture of the calcaneus and tarsal navicular. Radiol Case Rep. 2008;3:208.
- [CrossRef] [PubMed] [Google Scholar]
- Late reconstruction after navicular fracture. Foot Ankle Clin. 2006;11:105-19, ix
- [CrossRef] [PubMed] [Google Scholar]
- A literature-based guide to the conservative and surgical management of the acute Charcot foot and ankle. Diabet Foot Ankle. 2015;6:26627.
- [CrossRef] [PubMed] [Google Scholar]
- Posterior tibial tendon dysfunction: Its association with seronegative inflammatory disease. Foot Ankle. 1989;9:219-25.
- [CrossRef] [PubMed] [Google Scholar]
- Flat foot in a random population and its impact on quality of life and functionality. J Clin Diagn Res. 2017;11:LC22-7.
- [Google Scholar]
- Joint structure and function: A comprehensive analysis (4th ed). Philadelphia, PA: F.A. Davis Co.; 2005.
- [Google Scholar]
- Quality of life in adult population with flat feet. Int J Health Sci Res. 2020;10:193-200.
- [Google Scholar]
- Biomechanics and clinical analysis of the adult acquired flatfoot. Clin Podiatr Med Surg. 2007;24:617-44, vii
- [CrossRef] [PubMed] [Google Scholar]
- New radiographic parameters assessing forefoot abduction in the adult acquired flatfoot deformity. Foot Ankle Int. 2009;30:1168-76.
- [CrossRef] [PubMed] [Google Scholar]
- Tripod index: A new radiographic parameter assessing foot alignment. Foot Ankle Int. 2013;34:1411-20.
- [CrossRef] [PubMed] [Google Scholar]
- Spring ligament complex: MR imaging-anatomic correlation and findings in asymptomatic subjects. Radiology. 2005;237:242-9.
- [CrossRef] [PubMed] [Google Scholar]
- Posterior tibial tendon dysfunction as a cause of acquired flatfoot in the adult: Value of magnetic resonance imaging. Br J Rheumatol. 1997;36:136-9.
- [CrossRef] [PubMed] [Google Scholar]
- The effects of sectioning the spring ligament on rearfoot stability and posterior tibial tendon efficiency. J Foot Ankle Surg. 2008;47:219-24.
- [CrossRef] [PubMed] [Google Scholar]
- Acquired flatfoot in adults due to dysfunction of the posterior tibial tendon. J Bone Joint Surg Am. 1999;81:1173-82.
- [CrossRef] [PubMed] [Google Scholar]
- Biomechanical analysis of the three-dimensional foot structure during ait: A basic tool for clinical applications. J Biomech Eng. 2000;122:630-9.
- [CrossRef] [PubMed] [Google Scholar]




