
Translate this page into:
Imaging in elite and recreational cricket injuries: A pictorial review
 , Raj Ganeshan5, Rajesh Botchu2
, Raj Ganeshan5, Rajesh Botchu2
*Corresponding author: Rajesh Botchu, Department of Musculoskeletal Radiology, Royal Orthopaedic Hospital, Birmingham, United Kingdom. drrajeshb@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Kawthalkar AS, Shirodkar K, Ariyaratne S, Nischal N, Iyengar KP, Ganeshan R, et al. Imaging in elite and recreational cricket injuries: A pictorial review. J Arthrosc Surg Sports Med. 2024;5:84-9. doi: 10.25259/JASSM_25_2024
Abstract
Cricket is the second most popular spectator sport in the world after football, with an estimated fan base of 2.5 billion people and played professionally or semi-professionally in 108 countries. In the past two decades, with the establishment of newer formats such as Twenty-20, along with the traditional tests and one-day matches, there has been a significant rise in the amount and intensity of cricket being played. It has increased cricket-related injuries among elite athletes. With the rising popularity of cricket, there has also been a rise in cricket-related injuries among children, young adults and the so-called “weekend warriors.” Injuries in cricket can range from craniofacial trauma to lumbar stress injuries, abdominal wall strains, and various upper and lower extremity injuries. Musculoskeletal radiologists are vital to the sports medicine team involved in managing cricket injuries. There is a lacuna in current medical literature on a review of imaging in cricket injuries, and this article aims to address the same.
Keywords
Sports medicine
Musculoskeletal injuries
Cricket
Imaging

INTRODUCTION
Cricket is a ball sport played by 11 players on a team, involving significant technical skill, physical stamina, and tactical know-how. Cricket is a non-contact sport with three primary disciplines: batting, bowling, and fielding. Each discipline is characterized by its different physical stresses and biomechanics. It is played on a rectangular pitch in the center of a field, with the bowler throwing a hard ball at the batsman. The batsman aims to hit the ball with a wooden bat to score “runs.” The ten fielders (including the wicketkeeper behind the batsman) aim to stop or catch the ball and, thus, prevent the batsman from scoring runs.
Cricket is the second most popular spectator sport in the world after football, with an estimated following of 2.5 billion people. It is played at the highest (Test) level in 12 countries (designated full members of the International Cricket Council). The other shorter formats are played officially in 96 other countries (designated as associate members), highlighting the game’s global reach.
In the past two decades, there has been a significant increase in the amount of cricket played at the elite level, with the establishment of newer formats, a decrease in the rest interval between matches and an increase in the intensity of play associated with the newer (and also shorter) formats. It has increased cricket-related injuries among elite athletes. With the rising popularity of cricket, there has also been a rise in cricket-related injuries among children and young adults pursuing the game. Recreational cricket-associated injuries in so-called weekend warriors are also prevalent.
Cricketers can suffer a variety of injuries, from acute to chronic, including craniofacial trauma, lumbar stress injuries, abdominal wall strains, and various upper and lower extremity injuries.[1] These injuries are more common in bowlers, especially fast bowlers. Imaging plays a crucial role in the management of many of these injuries, and musculoskeletal radiologists are an integral part of the sports medicine team. This article aims to provide a comprehensive review of the imaging of the variety of injuries experienced by elite and recreational cricket players, ensuring that the readers are well-informed and knowledgeable.
CRICKETING INJURIES
Various cricketing injuries can occur in cricketers and are summarized anatomical region-wise in Table 1, and are discussed ahead in more detail.
| Upper limb injuries | Lower limb injuries |
|
|
| Thoracoabdominal and spinal injuries | Craniofacial injuries |
|
|
Craniofacial injuries
Although cricket is a non-contact sport, multiple impact injuries, including fractures, are common in it. These are most commonly due to the cricket ball in the head and neck region. The zygomatic bone is the most common facial bone to be fractured. Nasal bone fractures can also occur, as can soft tissue and bony orbital injuries.[2] Concussions occur in cricketers due to being struck by the cricket ball. Computed tomography (CT) or magnetic resonance imaging (MRI) of the brain is indicated in a patient with a concussion in the presence of red flag signs such as loss of consciousness, post-traumatic amnesia, focal neurological deficit, Glasgow coma scale of <15, and signs of clinical deterioration.[3,4]
Upper limb
Shoulder injuries are common in cricket.[5] These include rotator cuff tears, labral tears, glenohumeral dislocations resulting in Hill-Sachs and Bankart lesions, and biceps tendon tears. Chronic injuries such as rotator cuff tendinosis and acromioclavicular joint arthritis can also occur. Lateral and medial epicondylitis also occur in cricketers as chronic overuse injuries. Athletes with a predominantly posterior attachment of the biceps tendon to the labrum may be at increased predisposition for superior labrum from anterior to posterior tears.[6] An Australian study found a high prevalence of shoulder injuries in spin bowlers, followed by fast bowlers and fielders.[7]
Another injury seen in throwing athletes, including cricket fielders, is valgus overload syndrome, a triad of capitellar osteochondral injury or osteonecrosis, ulnar collateral ligament injury, and posterior elbow impaction injury.[1]
Wrist injuries include tendinosis of various flexor or extensor tendons. Triangular fibrocartilage complex injuries and injuries of the intrinsic or extrinsic ligaments of the wrist also occur [Figure 1]. Hand and finger injuries from ball impact are common in fielders and batsmen. Volar plate avulsion fractures are seen in fielders while trying to catch the ball, resulting from hyperextension from ball impact at the proximal interphalangeal joint, injuring the volar plate [Figure 1]. Various fractures of the fingers and thumb are common in cricketers, most common from impact from the cricket ball.[1] We also encountered a case of ulnar collateral ligament injury at the second metacarpophalangeal joint in an off-spin bowler, most likely from repeated motions of gripping and spinning the ball [Figure 1].
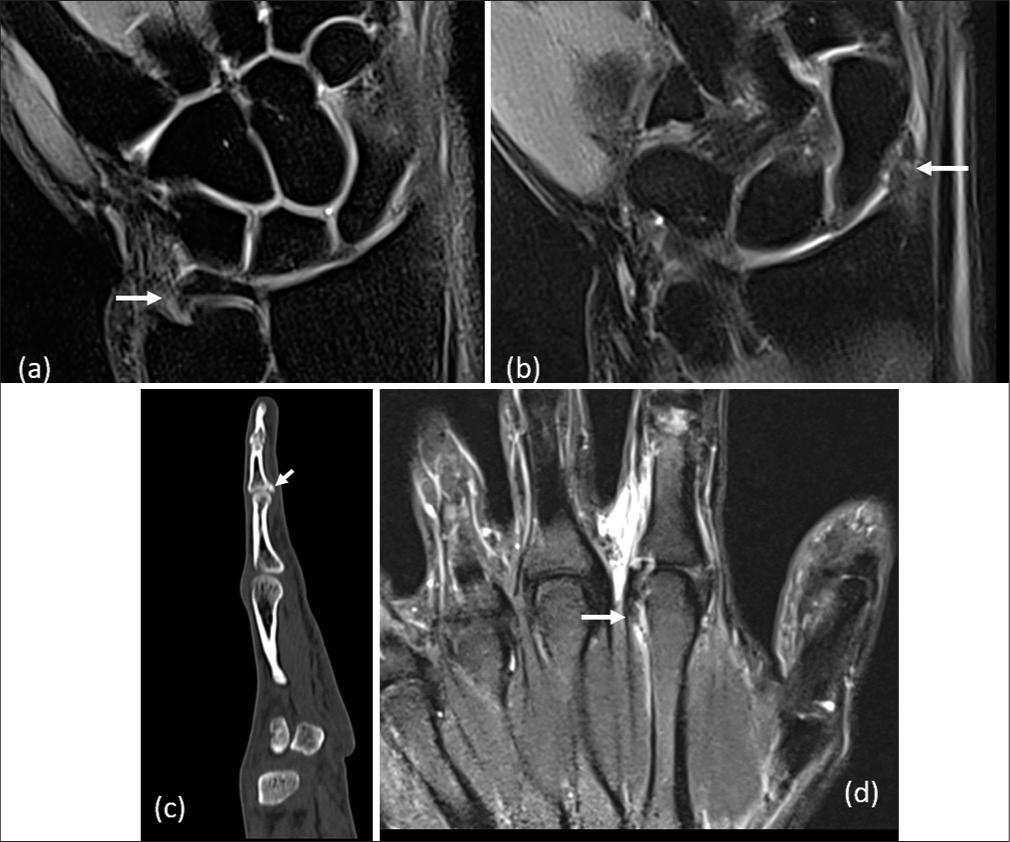
- Hand and wrist injuries in cricket. (a and b) Batsman with fall on outstretched hand while running between the wickets. Coronal proton density (PD) fat sat images show a complete tear of dorsal and volar radio-ulnar ligaments (a) and a complete tear of the radial collateral ligament (b) with mild edema in the adjacent radial styloid process (arrows). (c) The fielder with a hyperextension injury to the third finger while trying to catch the ball. The sagittal computed tomography image shows an avulsion fracture at the base of the middle phalanx with a fracture line extending into the proximal inter-phalangeal joint. This represents a volar plate avulsion fracture. (d) Off-spin bowler with long-standing pain in the second metacarpo-phalangeal joint. Coronal PD fat sat magnetic resonance imaging images show a partial tear of the ulnar collateral ligament of the second metacarpo-phalangeal joint, postulated to be a chronic overuse injury from spinning the ball (“Off-spinner’s finger”).
Thorax
Rib fractures can occur in cricket, as can various bruises and contusions from the cricket ball [Figure 2]. The rib injuries can be in the form of avulsion fractures associated with side strain or can be lower rib periostitis, which is an overuse injury causing thoracolumbar back pain. Both these injuries are common in cricket fast bowlers.[1]
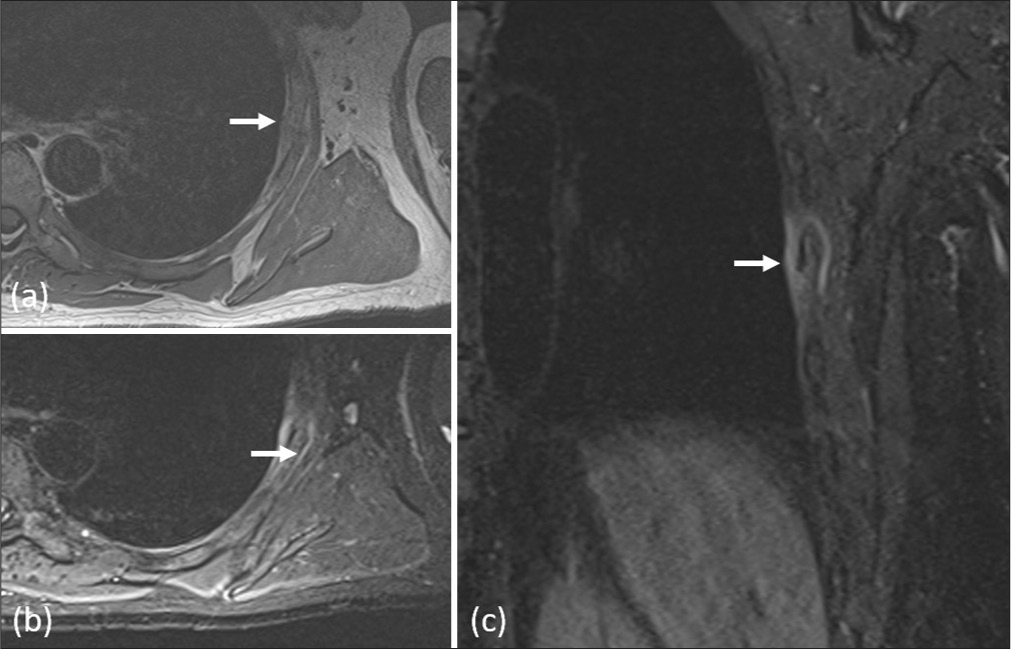
- Cricketer with left thoracic wall pain following impact from a ball while batting (such a ball being colloquially called a “rib tickler”). (a) Axial T1 image shows hypointensity in the left rib marrow. (b) and (c) Axial and coronal short-tau inversion recovery images show marrow edema in the rib with adjacent soft-tissue edema. The athlete had a linear, minimally displaced rib fracture.
Spine
A lumbar stress fracture is the most severe injury in modern cricket, resulting in a significant loss of playtime.[5] These are common in fast bowlers and usually occur opposite to the bowling arm [Figure 3]. These can be acute injuries or chronic ones due to overuse. The injury spectrum ranges from a stress reaction to incomplete stress fracture, complete stress fracture, and chronic stress fracture. Studies show the prevalence of these bony changes on MRI in 24–81% of fast bowlers.[1] An optimum imaging protocol will consist of T1 and T2 sagittal as well as short-tau inversion recovery images in two planes (sagittal and axial) to visualize bone marrow edema for stress reactions and T1VIBE sagittal.
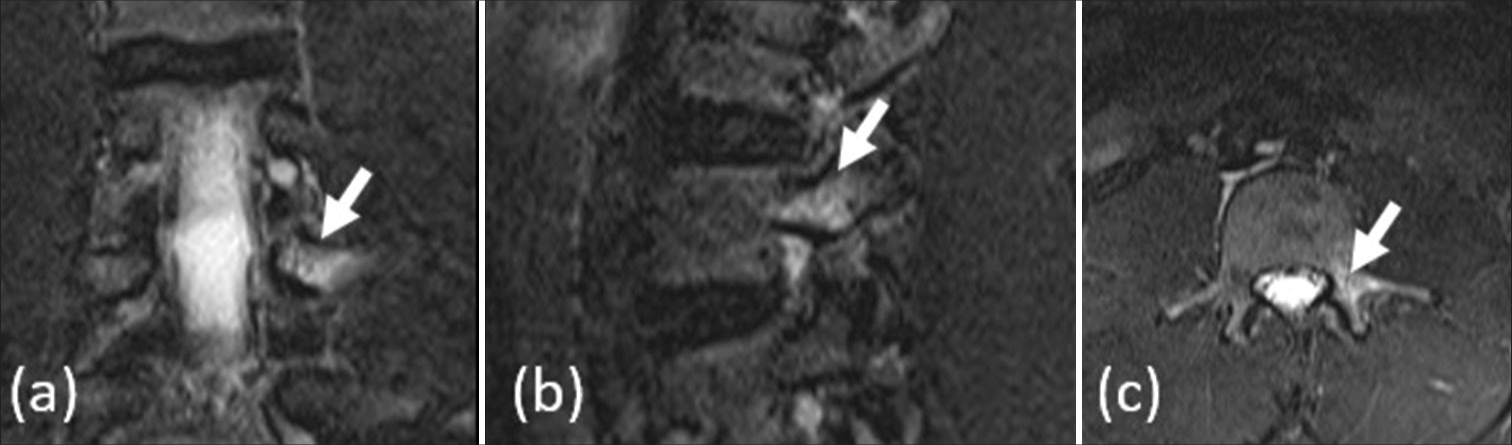
- Fast bowler with low back pain. (a) coronal, (b) sagittal, and (c) axial magnetic resonance imaging short-tau inversion recovery images demonstrate edema in the left pars interarticularis of L3 vertebra (white arrows), without cortical breach. This indicates a stress reaction of the pars interarticularis.
Abdominal wall and side strain
Side strains are common in elite cricketers, most commonly in fast bowlers, but also in batsmen and fielders. They usually occur on the side opposite to the bowling arm. They involve tears of the lateral abdominal wall muscles, with the most common muscle injured being the internal oblique. Injuries can occur near the ribs adjacent to the origin of the internal oblique or near the iliac crest attachment. Associated avulsion fractures of ribs are shown in Figure 4.[6] An ideal imaging protocol would include the lower three ribs till mid-pelvis in all three planes, with the axial and sagittal scans centered on the side of the pathology.
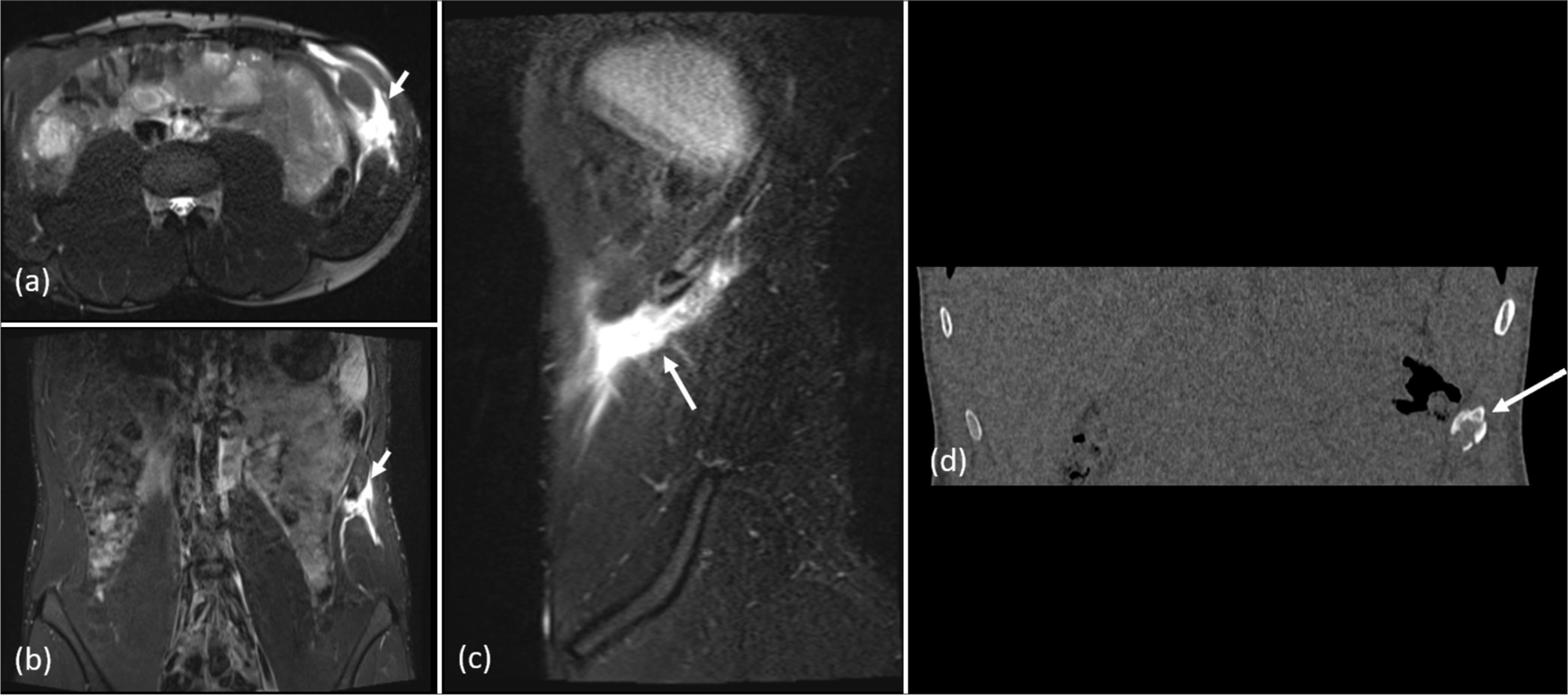
- Fast bowler with acute onset pain in the left lateral aspect of the abdomen. (a) axial, (b) coronal, and (c) sagittal magnetic resonance imaging short-tau inversion recovery images demonstrate a complete tear of the left internal oblique muscle near its origin from the lower ribs (white arrows). (d) Coronal computed tomography image shows an avulsion fracture of the left 11th rib at the site of attachment of internal oblique muscle (arrow).
Pelvis and groin
Athletic pubalgia is common in cricketers.[7] Rectus abdominis and adductor injuries can occur with or without marrow edema in pubic bone [Figure 5]. An optimum imaging protocol would focus on the rectus abdominis insertion-adductor origin region and pubic symphysis with short field-of-view images, with the inclusion of fat-saturated images to visualize muscle and bone marrow edema.
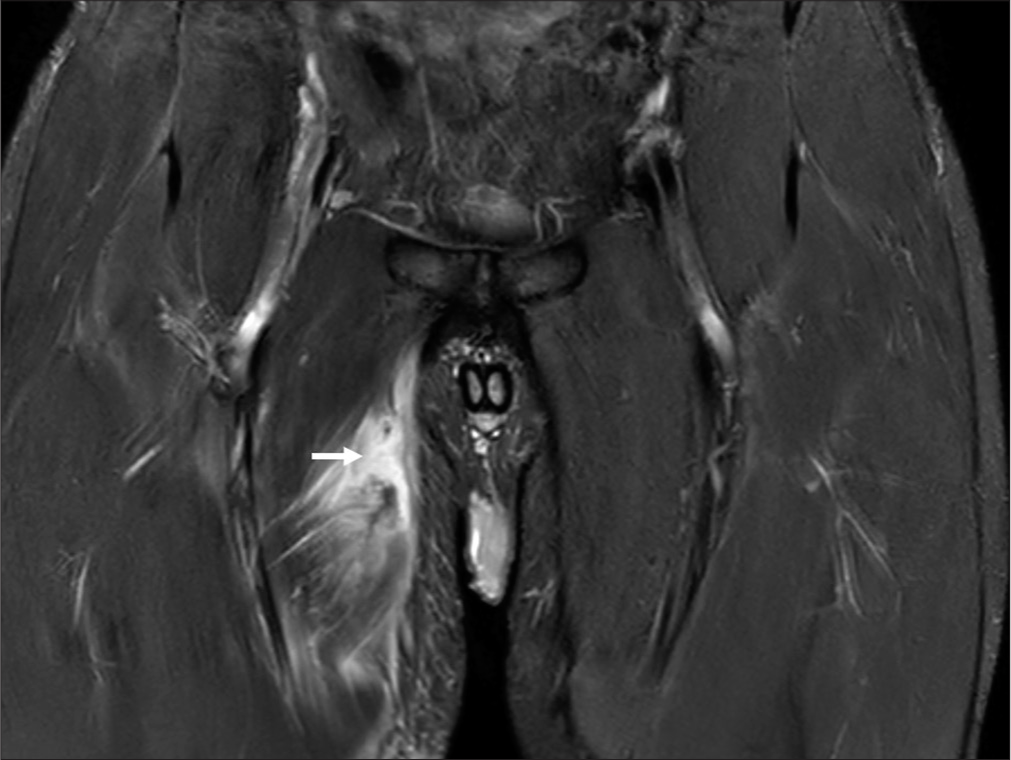
- Cricketer with right groin pain. Magnetic resonance imaging short-tau inversion recovery coronal image shows a complete tear of the right adductor longus muscle 4 cm below its origin, with complete separation of fibers and fluid signal intensity/hematoma (white arrow). There is edema in the adjacent muscle fibers.
Lower extremity
Hamstring injuries are the most common in modern cricket[1,8] [Figure 6]. MRI imaging protocol should include the ischial tuberosity to the knee to cover the hamstring tendon origin and insertion. The British Athletics Muscle Injury Classification is a commonly used classification for grading muscle injuries and estimating return to play.[9]
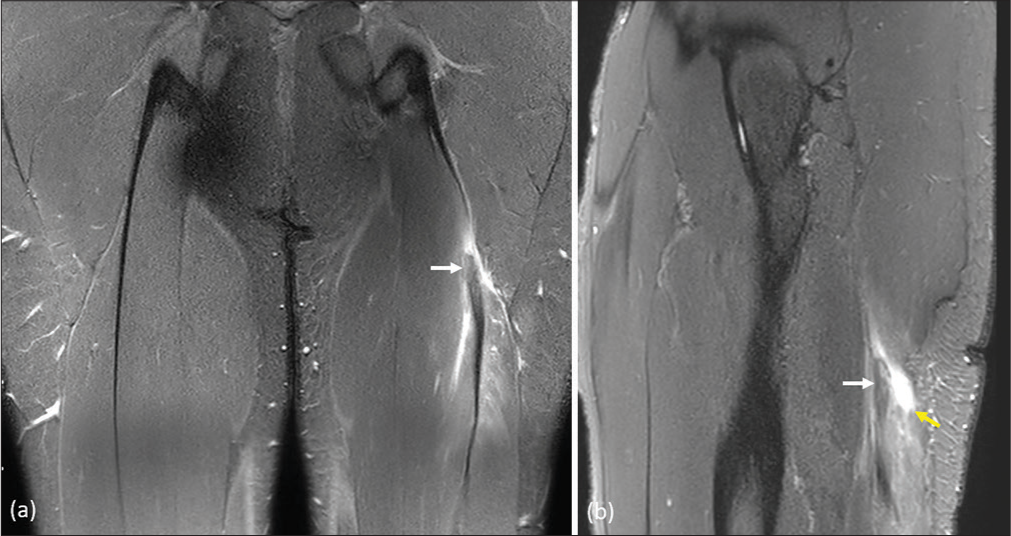
- Magnetic resonance imaging short-tau inversion recovery (a) coronal and (b) sagittal images respectively, in a cricketer with posterior thigh pain. These show edema with fluid signal intensity (yellow arrow) in the biceps femoris muscle with thickening and hyperintensity within its tendon (white arrow). British athletics muscle injury classification grade 2c injury.
Tibial stress fractures and stress reactions occur commonly in bowlers, batsmen, and fielders, usually along the medial tibial cortex [Figure 7]. Imaging helps to evaluate the severity of these injuries and grade them, which helps the treating physician and physiotherapist estimate return to play. The Fredericson classification is commonly used to grade medial tibial stress injuries.[10]
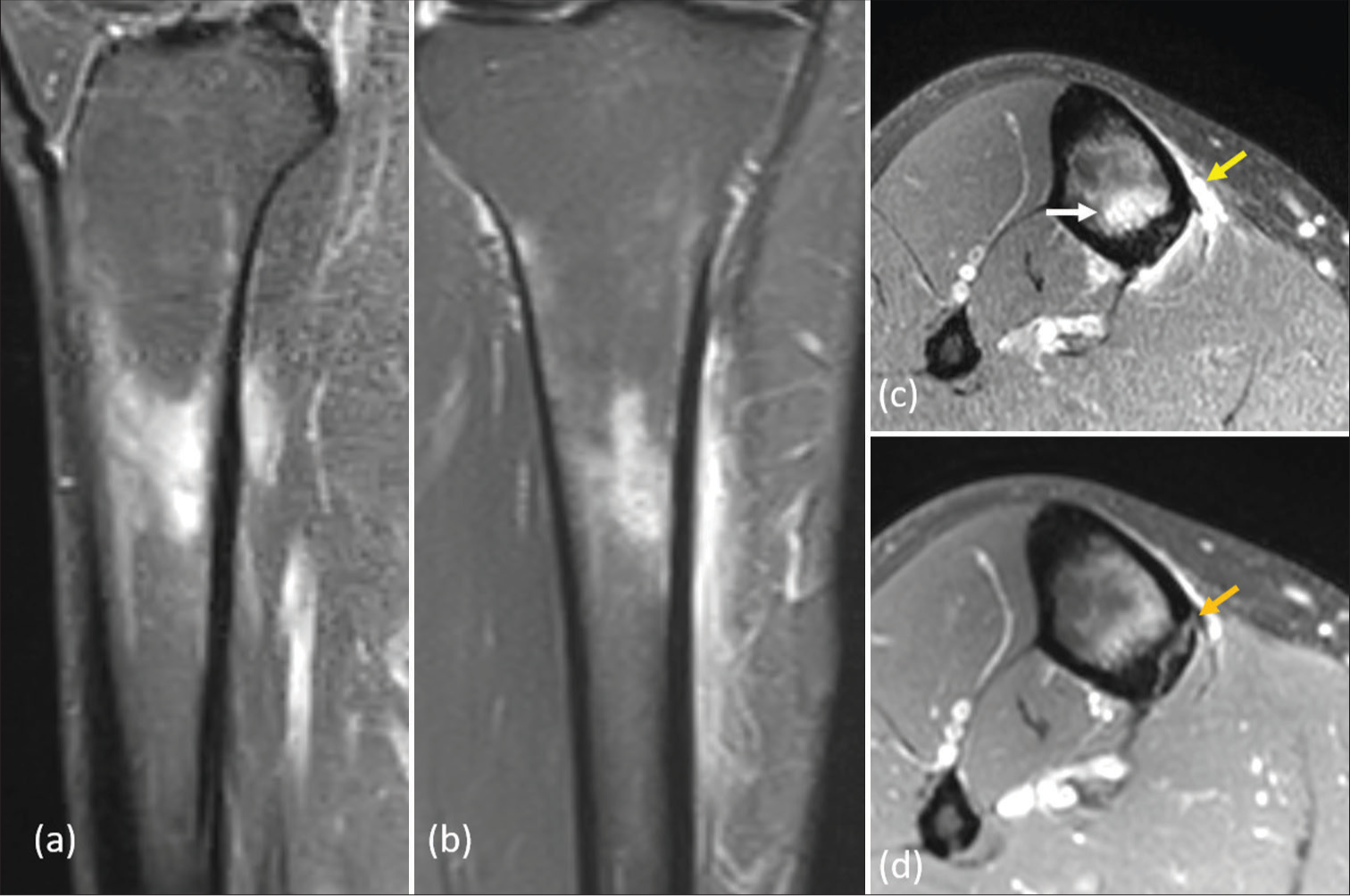
- Magnetic resonance imaging short-tau inversion recovery (a) sagittal, (b) coronal, (c) and (d) axial images respectively, in a cricketer with pain in the right anteromedial leg. Marrow edema (white arrow) and subperiosteal edema (yellow arrow) in tibia with cortical linear hyperintensity (orange arrow). Fredericson grade 4b tibial stress injury (in this case a stress fracture).
Patellar tendinopathy, iliotibial band friction syndrome, and chondral degeneration are overuse injuries of the knee seen in cricketers [Figure 8]. Knee ligament tears and meniscal injuries occur but are less common than in football. Most of the anterior cruciate ligament and meniscal injuries are reported to occur in fielding while diving to catch the ball.[11] Knee collateral ligament injuries usually occur in bowlers when the knee is twisted on a fixed foot during bowling.[12]
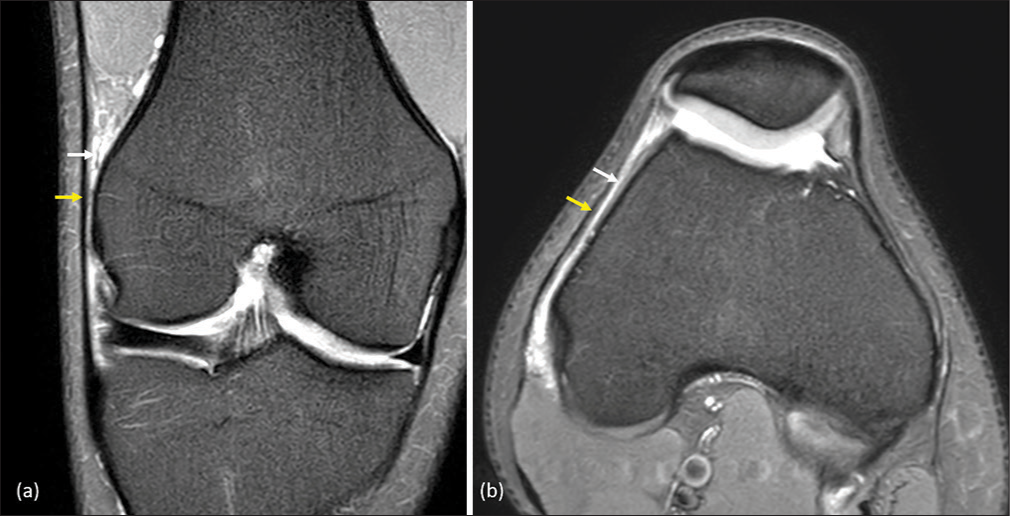
- Cricketer with pain along the lateral aspect of the knee. Magnetic resonance imaging proton density fat sat (a) coronal and (b) axial images show edema (white arrow) in the soft tissues deep to the iliotibial band (yellow arrow). These findings indicate iliotibial band friction syndrome.
Ankle ligament injuries also occur, along with anterolateral and posterior ankle impingements. Posterior ankle impingements are common in fast bowlers and can be associated with ankle synovitis, os trigonum disorders, and flexor hallucis longus tendinosis. Acute injuries are more common in the forefoot during sagittal movements, such as in bowling, while chronic overuse injuries and instability are more common in the hindfoot.[1]
ROLE OF MUSCULOSKELETAL INTERVENTIONS
Various image-guided musculoskeletal interventions help treat many acute and chronic cricket-related injuries. Intra-articular, bursal, and tendon sheath injections can be performed for various chronic injuries. Chronic lateral epicondylitis can be handled with imaging guidance. Upper and lower limb nerve entrapments can be treated with hydrodissection.
UNCOMMON INJURIES
Specific uncommon injuries reported in cricket are vertebral artery dissection because of cricket ball impact and testicular rupture. We encountered a lower limb compartment syndrome case in an elite cricketer [Figure 9]. Medial gastrocnemius tear (also known as “tennis leg”) can also be seen in cricket [Figure 10]. Complete biceps tendon tears are rare and usually seen in cricketers performing weight-lifting activities at the gym.
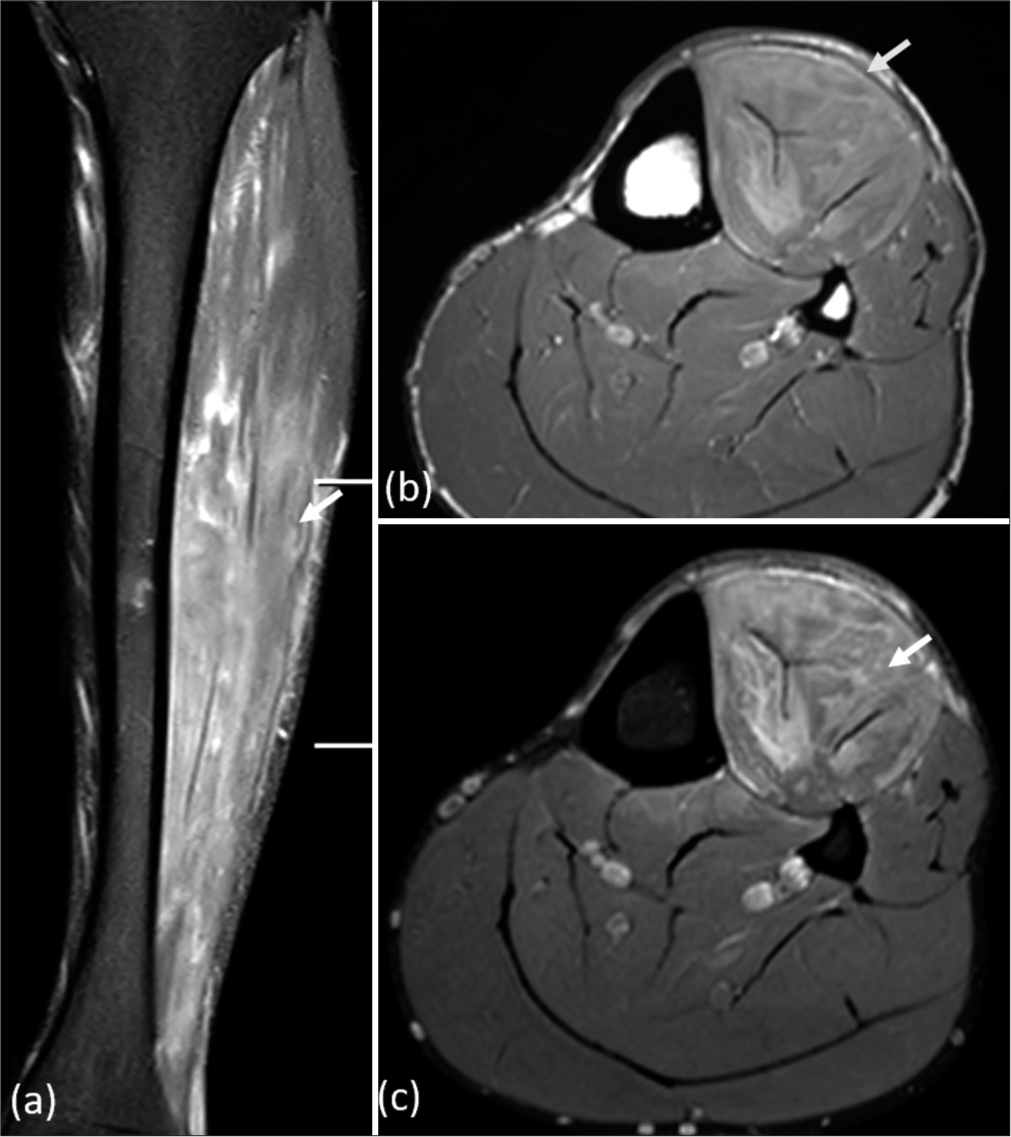
- Magnetic resonance imaging short-tau inversion recovery (STIR) (a) coronal, (b) axial T1, and (c) axial STIR images respectively, show anterior bowing of the anterior compartment fascia (yellow arrow), with significant edema within the anterior compartment muscles (white arrow). These findings indicate acute compartment syndrome.
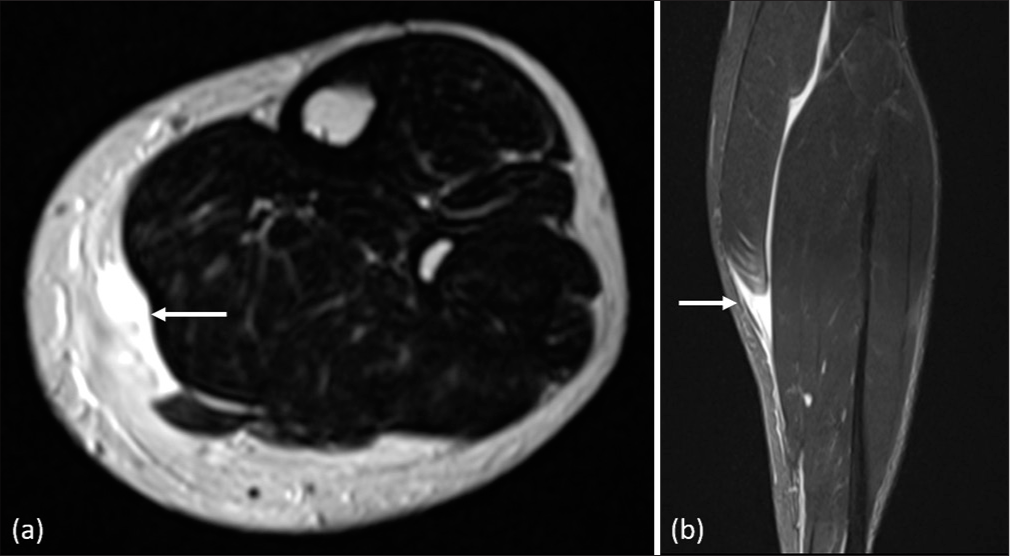
- Batsman with a calf injury while running between the wickets. Axial T2 (a) and coronal short-tau inversion recovery (b) magnetic resonance imaging images show a complete tear of medial gastrocnemius with retraction of fibers till mid-calf, also called “tennis leg.”
DIFFERENCES BETWEEN ELITE AND RECREATIONAL CRICKET INJURIES
While both elite and recreational cricket players are susceptible to injuries, the nature and frequency of these injuries can differ significantly due to factors such as intensity of play, protective equipment, physical conditioning, biomechanics, and medical support. Table 2 presents the differences between elite and recreational cricket injuries.
| Factor | Elite cricket | Recreational cricket |
|---|---|---|
| Intensity and Frequency of Play | High-intensity, frequent matches | Lower intensity, less frequent matches |
| Protective Equipment | Top-quality gear, helmets, pads, gloves | Limited protective gear |
| Physical Conditioning | High level of fitness, strength, speed, endurance | Varying levels of fitness |
| Biomechanics | Refined movement patterns | Less refined movement patterns |
| Medical Support | Access to top-notch sports medicine specialists | Limited access to medical care |
CONCLUSION
Cricket, despite being a non-contact sport, is prone to various injuries due to the intense physical demands and repetitive movements involved. From craniofacial trauma to lower extremity injuries, cricketers face a wide spectrum of musculoskeletal ailments. Imaging modalities, particularly MRI, play a crucial role in diagnosing and guiding the management of these injuries. Musculoskeletal radiologists are indispensable members of the sports medicine team, ensuring accurate diagnosis and appropriate treatment. By understanding common injuries and imaging techniques, healthcare professionals can provide effective care to cricketers at all levels, promoting their well-being and longevity in the sport.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent was not required as there are no patients in this study.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- A systematic review of head, neck and-facial injuries in cricket. Int J Sports Med. 2022;43:496-504.
- [CrossRef] [PubMed] [Google Scholar]
- Imaging of concussion in young athletes. Neuroimaging Clin N Am. 2018;28:43-53.
- [CrossRef] [PubMed] [Google Scholar]
- International Cricket Council. 2020. Available from: https://resources.pulse.icc-cricket.com/icc/document/2021/01/21/28d8425f-cbc6-4101-b336-e567fdabc737/icc-concussion-management-guidelines-dec-2020.pdf [Last accessed on 2024 Jun 12]
- [Google Scholar]
- Activity specific areal bone mineral density is reduced in athletes with stress fracture and requires profound recovery time: A study of lumbar stress fracture in elite cricket fast bowlers. J Sci Med Sport. 2022;25:828-33.
- [CrossRef] [PubMed] [Google Scholar]
- Side strain in sport: A narrative review of pathomechanics, diagnosis, imaging and management for the clinician. J Sci Med Sport. 2017;20:261-6.
- [CrossRef] [PubMed] [Google Scholar]
- Sports hernia or groin disruption injury? Chronic athletic groin pain: A retrospective study of 100 patients with long-term follow-up. Hernia. 2014;18:815-23.
- [CrossRef] [PubMed] [Google Scholar]
- Hamstring injuries in England and Wales elite men's domestic cricket from 2010 to 2019. J Sci Med Sport. 2022;25:474-9.
- [CrossRef] [PubMed] [Google Scholar]
- British athletics muscle injury classification: A new grading system. Br J Sports Med. 2014;48:1347-51.
- [CrossRef] [PubMed] [Google Scholar]
- Tibial stress reaction in runners. Correlation of clinical symptoms and scintigraphy with a new magnetic resonance imaging grading system. Am J Sports Med. 1995;23:472-81.
- [CrossRef] [PubMed] [Google Scholar]
- Acute anterior cruciate ligament injuries in multisport elite players: Demography, association, and pattern in different sports. J Clin Orthop Trauma. 2016;7:187-92.
- [CrossRef] [PubMed] [Google Scholar]
- Cricket injuries: An orthopaedist's perspective. Orthop Surg. 2014;6:90-4.
- [CrossRef] [PubMed] [Google Scholar]




