
Translate this page into:
Arthroscopic intercruciate trans-septal posterior cruciate ligament avulsion fixation with pull-through technique using a single button adjustable loop device

*Corresponding author: Himanshu Gupta, Sports Injury Centre, Vardhman Mahavir Medical College and Safdarjung Hospital, Delhi, India. himanshu.aiims@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Gupta H, Mittal BS, Jain V. Arthroscopic intercruciate trans-septal posterior cruciate ligament avulsion fixation with pull-through technique using a single button adjustable loop device. J Arthrosc Surg Sports Med. 2024;5:125-29. doi: 10.25259/JASSM_15_2024
Abstract
Numerous arthroscopic techniques have been described for the fixation of posterior cruciate ligament avulsion, including the pull-out technique with suture or tape fixed with a knot tied over a free cortical button on the anterior tibial cortex, and the adjustable loop with double cortical buttons. We present a modification of the suture pull-out method utilizing the readily available adjustable loop with a single cortical loop button for fixation on the anteromedial tibial cortex. The surgery is performed through an intercruciate trans-septal approach with the suture bridge configuration and cross-over of suture tapes, with two diverging tibial tunnels with a single anterior opening forming a “Y-shaped tunnel.” The advantages of the suture pull-through method and the adjustable loop device can be combined using this technique modification.
Keywords
Posterior cruciate ligament
Avulsion
Adjustable loop
Arthroscopic
Fixation

INTRODUCTION
Numerous arthroscopic techniques have been described for the fixation of posterior cruciate ligament (PCL) avulsions, which vary according to the portals utilized, the number of bone tunnels, and the fixation method.
The pull-out technique is commonly used for arthroscopic PCL avulsion fixation.[1] A suture or tape looped around the PCL is fixed with a knot tied over a free cortical button on the anterior tibial cortex, with either a single or two tibial tunnels. However, we believe from our experience that slight loosening of the knot at the time of tying, leading to inadequate seating or displacement of the PCL avulsion fragment on its bony bed, is not unusual and may result in per-operative failure.
Another technique utilizes an adjustable loop with double cortical buttons[2,3] (e.g., the Syndesmotic Tightrope, Arthrex). Certain limitations exist for this procedure. First, the reduction of the avulsed fragment before reaming the tunnel is essential, otherwise, the fragment may not fully sit in place once the button is passed. Second, drilling through the avulsed fragment may cause it to shatter into smaller bony fragments. Third, this technique cannot be employed with severely comminuted avulsions as there are higher chances of the button cutting through the fragment.
We present a modification of the suture pull-out method utilizing the readily available adjustable loop with a single cortical loop button for fixation on the anteromedial (AM) tibial cortex. The procedure is performed through an intercruciate trans-septal approach[4] with the suture bridge configuration and cross-over of suture tapes,[5] with two diverging tibial tunnels with a single anterior opening (“Y-shaped tunnel”). The advantages of the suture pull-through method and the adjustable loop device can be combined using this technique modification. The index case was a 32-year-old male with an isolated acute avulsion injury of PCL with no external wound and no neurovascular deficit.
SURGICAL TECHNIQUE
The patient is positioned supine under general or spinal anesthesia with the operative limb hanging off the side of the operating table, and a thigh tourniquet is inflated.
The standard anterolateral (AL) and high AM portals are established, and an arthroscopic evaluation is performed using a 30° arthroscope. The intercruciate window is then opened with a motorized shaver and a radiofrequency (RF) probe.[4] [Video 1] The posteromedial (PM) portal is created using standard techniques.
Video 1:
Video 1:Video demonstrating the surgical technique of arthroscopic intercruciate transseptal posterior cruciate ligament avulsion fixation with pull-through technique using a single button adjustable loop device.Thus, two visualization windows are created for the posterior compartment- one between the PCL and the lateral border of the medial femoral condyle (modified Gillquist view), and the other through the intercruciate region. By alternating a 70° arthroscope between these two windows, the posterior septum is cleared using an RF probe inserted from the PM portal. A Wissinger rod is inserted from the PM portal toward the posterolateral (PL) compartment, creating the PL portal. This rod is utilized from the PL portal to elevate the posterior capsule and aid in visualization. The fracture fragment is identified, and the surrounding area is cleared. The gap is freshened with a tissue liberator if not a recent fracture. The location of the fragment and adequacy of preparation is also confirmed by visualization from the PM portal.
While visualizing from the AL portal through the intercruciate region, the femoral PCL guide (Arthrex, Germany) set at 70° is inserted through the PM portal and placed on the posterior tibia, distal, and lateral to the fragment bed. Through this, the lateral tibial tunnel is drilled with a Beath pin followed by a 4.5 mm reamer [Figure 1a]. The femoral PCL guide is used instead of the tibial PCL guide as it provides a better approach through the PM portal. Then, this drill guide is placed distal and medial to the bed, and through the same anterior cortical drill hole, the medial tibial tunnel is drilled [Figure 1b]. Thus, two posterior tibial tunnels are created with a confluent single anterior hole. It is ensured that the tip of the bone bridge at the point of diversion of the two tunnels lies at least 15 mm from the anterior cortex so that the shortened adjustable loop can be accommodated and there is scope for additional pulling of the PCL sutures (see later). This is ensured by inserting a 4.5 mm reamer in the center of the anterior tunnel until the 15 mm mark has passed the anterior cortex [Figure 2]. Thus, a Y-shaped tunnel is formed. One shuttling suture each is then placed in the medial and lateral tunnels out from the PM portal. By alternating visualization between the intercruciate approach and the modified Gillquist view, a polyethylene suture and a polyethylene tape (XBraid TT and Force Fiber, Stryker, USA) are looped around the PCL base just above the avulsed fragment, with both ends of the suture and the tape exiting through the PM portal. For obtaining suture bridge configuration, the fixation sutures can be crossed over at the back of PCL, with the medial end shuttled through the lateral tibial tunnel and vice versa. Another way of obtaining a suture bridge configuration is to tie a loose knot on the two ends of the fixation suture to lie on the middle of the back of the PCL fragment and then pass the two ends of the suture through the two different tunnels. In the present index case, both methods have been used. A loose Duncan knot is placed in the polyethylene suture to lie over the posterior aspect of the fragment. One end of the polyethylene suture and the medial end of the tape are shuttled through the lateral tibial tunnel using the polyester suture, and the other end of the suture along with the lateral end of the tape are shuttled through the medial tibial tunnel, thus creating a cross-over of the suture tape. By pulling on the suture and the tape, the reduction is achieved and also visualized from the PM portal. After this, the loop of an adjustable loop button (Procinch RT, Stryker, USA) is placed between the two ends of the suture and tape, and the suture and tape are tied securely over the cancellous bridge inside the tunnel at the level of confluence of the two tunnels, using multiple alternating half hitches using a knot pusher, thus creating a linkage between the adjustable loop and the suture-tape which were looped around the PCL [Figure 3a]. The ends of the polyethylene suture and tape can be passed through the button for additional fixation at the end of the procedure. After this, the adjustable loop is shortened along with an anterior drawer force, placing the button on the anterior cortex and further pulling on the knot of the polyethylene suture and tape [Figure 3b]. Thus, further distal pulling of the avulsion fragment is achieved by this as needed. This reduction is visualized from the PM portal as well as using the C-arm [Figure 4] and is further confirmed in the form of tightening of both the anterior cruciate ligament and the PCL visualized from the AL portal. Finally, the ends of the polyethylene suture and tape that were brought through the button are further tied over it for secondary or additional fixation. After the closure of incisions, a posterior tibial support (PTS) brace is given.
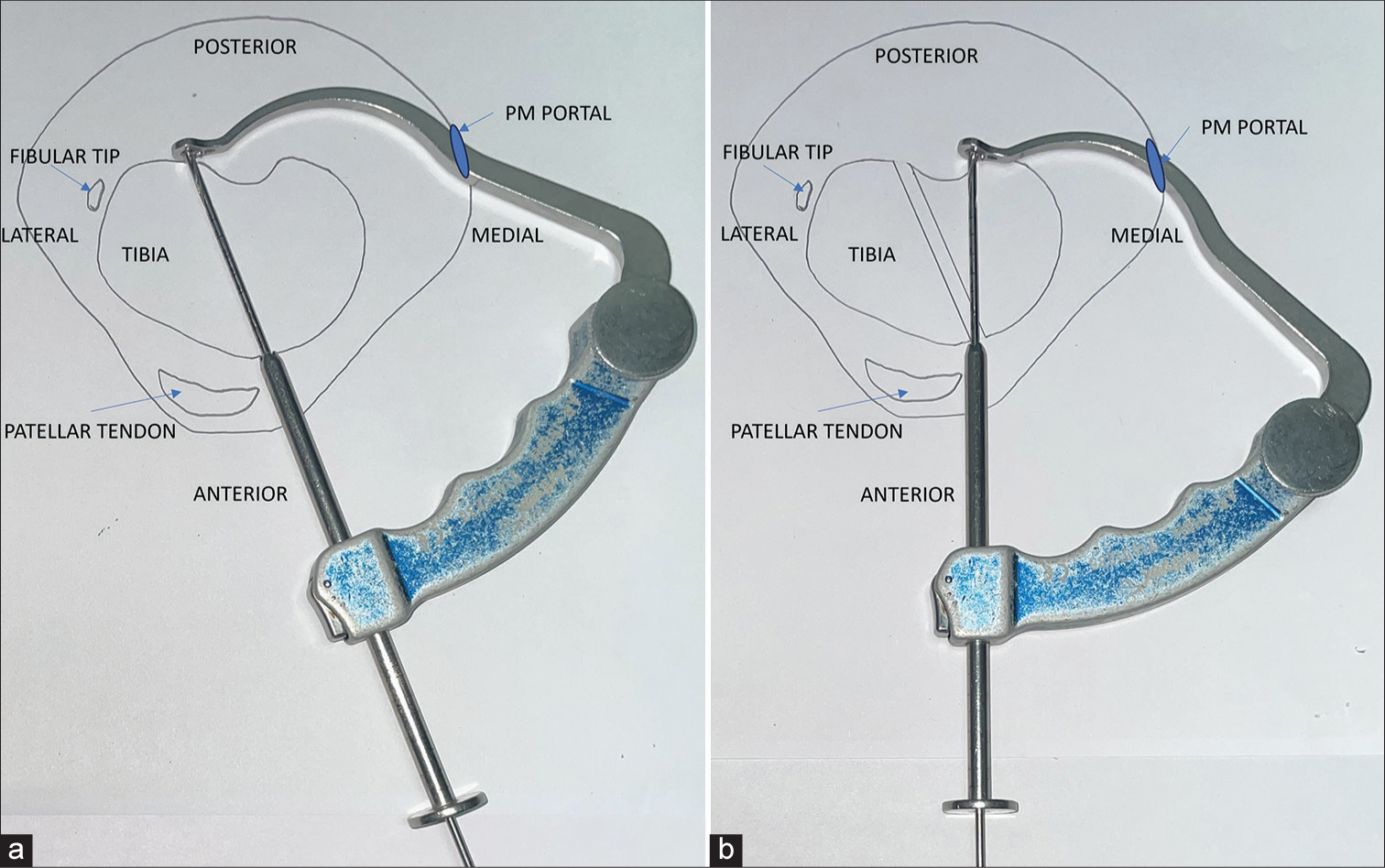
- (a and b) Drawing of axial section of the proximal tibia showing placement of the posterior cruciate ligament femoral drill guide over posterior tibia through the posteromedial portal for drilling the medial and lateral tibial tunnels with the single anterior opening.
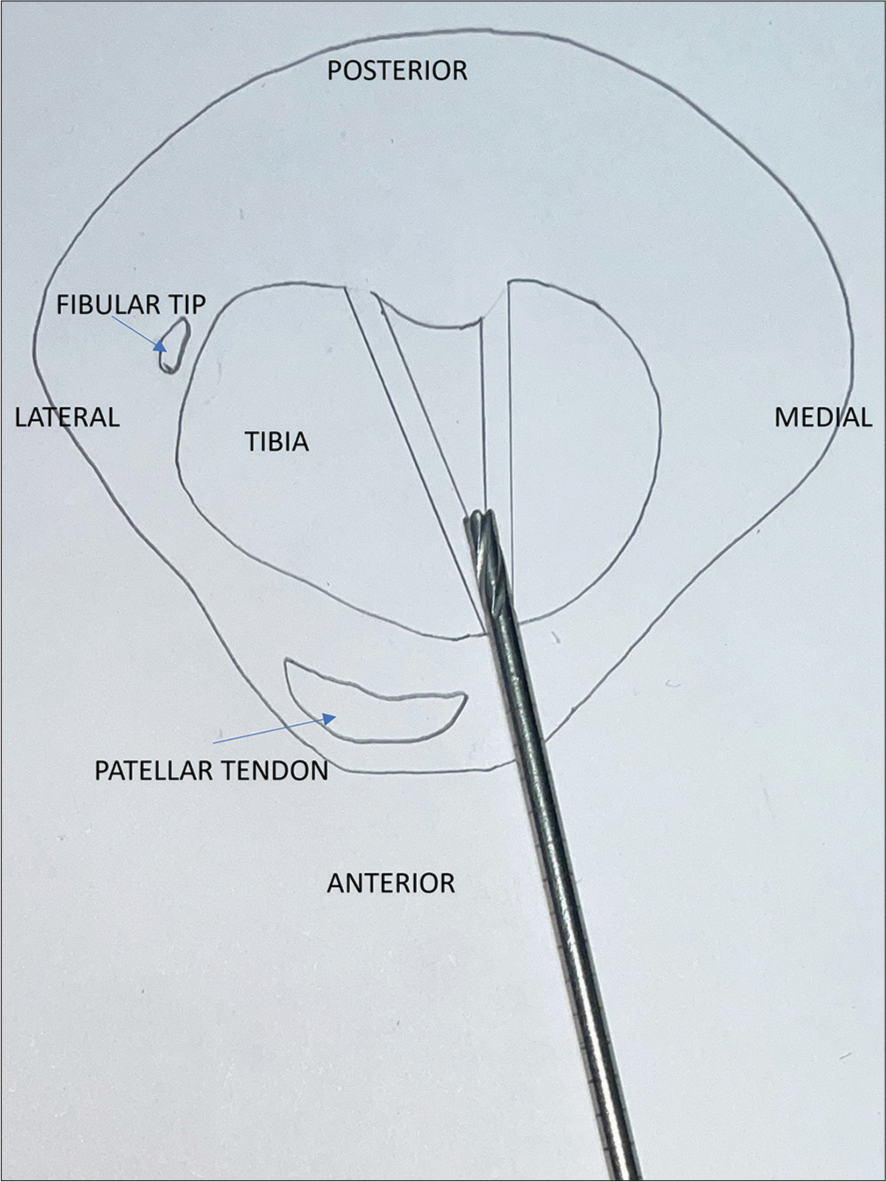
- It is ensured that the cancellous bone bridge lies at least 15 mm deep from the anterior cortex (see text), by inserting a 4.5 mm reamer in the center from the anterior opening of tunnels.
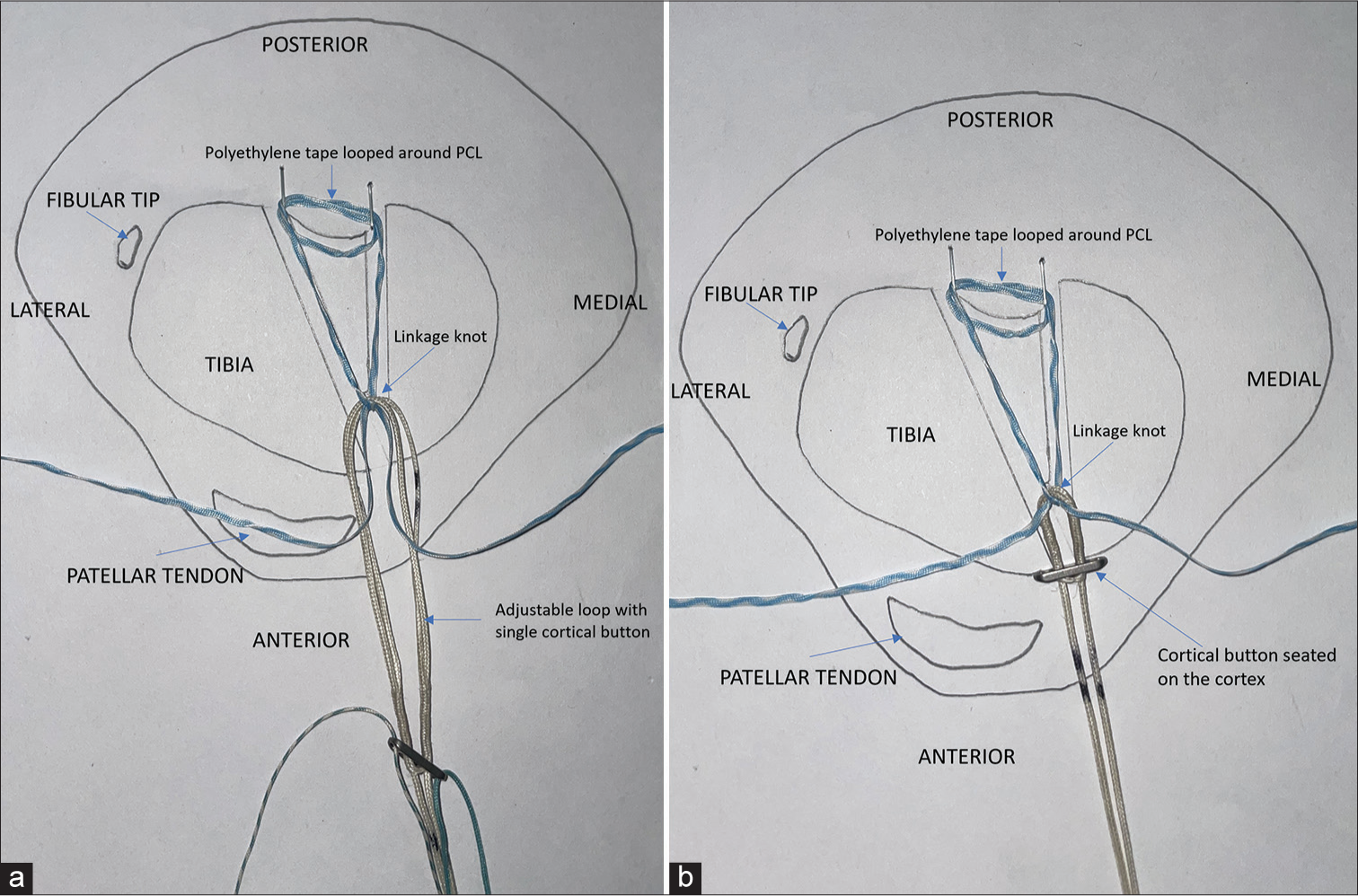
- (a) A secure non-sliding knot linkage is created between the polyethylene tape/sutures that were looped around the posterior cruciate ligament (PCL) and the adjustable loop. This knot lies on the cancellous bridge, pushing the adjustable loop at least 15 mm inside the tunnel. Please note that for the sake of clarity, only one tape has been shown to be looped around the PCL and the polyethylene suture has not been shown in these diagrams. (b) The Adjustable loop has been shortened, placing the critical button on the cortex and pulling on the PCL fragment to reduce it.
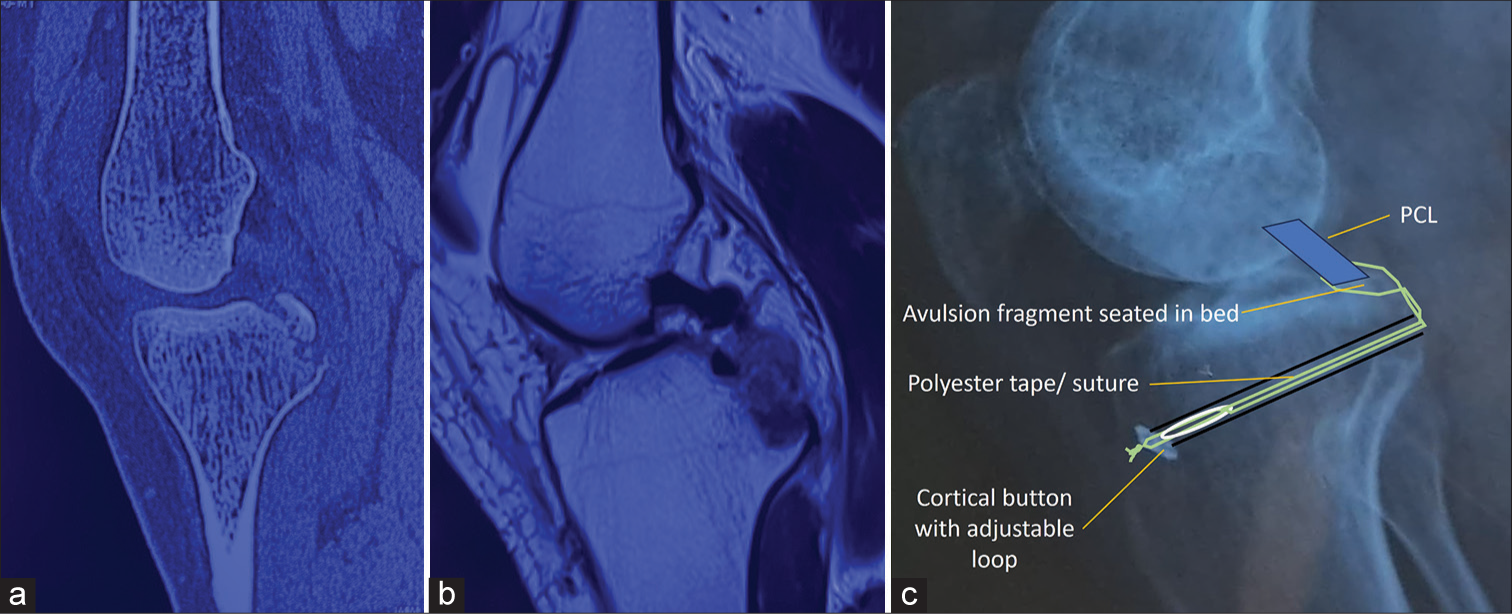
- (a) Pre-operative sagittal section of computed tomography and (b) magnetic resonance imaging showing the posterior cruciate ligament avulsion. (c) Follow-up X-ray at six months with a bony union, showing the configuration of the tape-loop-button construct. PCL: posterior cruciate ligament.
Post-operative rehabilitation is standard. The patient is kept non-weight bearing for six weeks with a PTS brace and crutches. Range of motion (ROM) of 90° is achieved by six weeks. After six weeks, partial weight-bearing is progressed to full weight-bearing, and the brace is discontinued after 8–10 weeks. Open chain exercises are added at six weeks. Regular X-rays are done to look for union or displacement. Our index case showed complete union at three months and full ROM and return to all activities at the short-term follow-up of six months.
DISCUSSION
In this technical note, we have presented a modification of the suture pull-out fixation method for PCL avulsions. It utilizes the intercruciate trans-septal approach,[4] along with the suture bridge configuration with cross-over of suture tapes,[5] which are already described. A fixation method with two diverging tibial tunnels with a single anterior opening (“Y-shaped tunnel”), along with final fixation with a single button-adjustable loop, has been added, creating a tape-loop-button construct [Figure 3b and 4]. Thus, the advantages of the suture pull-through method and the adjustable loop device have been combined.
The adjustable loop button allows for the controlled reduction of the fragment and prevents intraoperative loosening that may otherwise occur while tying standard knots over a cortical button on the anterior cortex.[1,6] It may be noted that the knot placed on the soft cancellous bridge inside the tunnel was only to create a link between the polyethylene tape and the loop-button device. When the adjustable loop is shortened, it pulls on the knot placed on the polyethylene tape, thus pulling it away from the cancellous bridge and removing any laxity in the tape that may have crept in while tying the knot. Hence, in the end, the stability in the construct is provided by the button resting on the anterior cortex, and the shortening of the adjustable loop achieves the tension. Multiple studies have reported on the use of a two-button adjustable loop device, emphasizing its efficacy but noting potential complications with fragment reduction and drill-induced fragment damage. These potential complications are mitigated by our technique. The advantages of this technique over the double button shortening loop technique are that, first, it is not necessary to hold the avulsed fragment in a reduced position at the time of drilling. Second, drilling is not done through the avulsed fragment, so the risk of further breaking the fragment is mitigated.[2,3]
A pull-out technique using a suture or tape looped around the PCL and fixed through a single tibial tunnel over a free cortical button using a standard knot is described in literature.[1] However, there are potential issues with knot security resulting in fragment displacement, both intraoperatively as well as later. Our present technique modification addresses these issues with the adjustable loop device.
The suture bridge configuration involving crossing over of the fixation tape or suture over the PCL and passage through two different tibial tunnels, one medial to and one lateral to, the avulsion crater, was described by Yoon et al.[5] In their technique, two tibial tunnels (with two anterior and two posterior openings) were drilled, and the fixation was done over the cortex between the anterior openings. The technique has all the potential issues of knot security and fragment displacement as with any pull-out technique. However, their concept of suture bridge configuration with two tibial tunnels was utilized in our current technique.
Tang and Zhao described a technique with two tibial tunnels in which the pull-through sutures were tied over the cortical bridge, and in addition, a supplementary fixation was added by linking these sutures with an adjustable loop-button construct passed through a third tibial tunnel.[7] However, this technique required the drilling of a third horizontal tibial tunnel, thus creating four cortical holes in the medial and lateral tibial cortices. In contrast, in our technique, only one anterior hole is created in the medial tibial cortex. Further, the use of widely available surgical tools and implants increases the potential applicability of our technique in various settings. In the index case, as well as in the other cases in which the authors have used the current technique, the authors did not find any difficulty in creating the Y-shaped tunnels. The entry point for the second drill pin lies on the cancellous wall of the first tunnel, and to prevent its slippage at the time of drilling, the trick is to use a stiff 2.4 mm Beath pin and first push it or gently hammer it into the cancellous wall of the first tunnel in the desired direction through the jig, and then attach the drill machine. Subsequently, there is no specific jig for drilling off the bone bridge to a depth of 15 mm and this step depends on the control of the surgeon on the drill machine, but it is not difficult to perform. Further, the adequacy of the removal of the bone bridge to 15 mm depth can be ensured by probing the stem of the Y-tunnel with a probe.
The need to remove the bone bridge to 15 mm depth is based on two reasons – first, to accommodate the loop length after maximum shortening of the adjustable loop, which, for the commonly available brands, varies from about 8–12 mm (personal measurements). Second, additional space is required to allow distal pulling of the knot of the fixation tape (along with the fragment) at the time of shortening of the adjustable loop.
At the short-term follow-up of 6 months, our index case showed complete union and return to all activities. However, given the sample size of one, it is impossible to draw definitive conclusions about the efficacy of this technique modification vis-a-vis the conventional techniques. Future studies should include a larger sample size with appropriate power analysis to detect clinically significant differences and validate the findings of the current report. Longer-term follow-up of more than two years is also needed to look at the final functional outcomes and long-term complications of this technique.
Indications of this technique
The indications for this surgery are an acute bony avulsion fracture of the PCL from tibial attachment.
Limitations of this technique
Contraindications include an associated mid-substance injury to PCL and vascular injuries needing an open approach. In addition, old avulsions may not be amenable to arthroscopic fixation, although the same fixation method may be utilized after open reduction and freshening of the bone bed.
How to avoid complications
The length of the combined single tunnel anteriorly should be at least 15 mm to allow for the minimum length of the shortened adjustable loop and for further pulling of the polyethylene tape. Suture management should be appropriate to avoid suture tangling. The reduction should be checked directly from the PM portal as well as under C-arm.
CONCLUSION
To conclude, we have presented in this technical note a modification of the suture pull-out fixation method for PCL avulsions using a single-button adjustable loop device, which combines the advantages of the suture pull-through method and the adjustable loop.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Clinical experience with arthroscopic suture pull technique in isolated PCL avulsion injuries. J Clin Orthop Trauma. 2020;11(Suppl 3):S362-7.
- [CrossRef] [PubMed] [Google Scholar]
- Short-term clinical outcomes of arthroscopic fixation of displaced posterior cruciate ligament avulsion fractures with the use of an adjustable loop suspensory device. J Orthop Surg Hong Kong. 2019;27(2) [Last accessed on 2024 May 23]
- [CrossRef] [PubMed] [Google Scholar]
- Adjustable-loop cortical button fixation results in good clinical outcomes for acute tibial avulsion fracture of the posterior cruciate ligament. Arthrosc Sports Med Rehabil. 2023;5:e307-13.
- [CrossRef] [PubMed] [Google Scholar]
- Intercruciate trans-septal arthroscopic approach to the posterior compartment of the knee joint. J ISAKOS. 2023;8:502-8.
- [CrossRef] [PubMed] [Google Scholar]
- Arthroscopic suture bridge fixation technique with multiple crossover ties for posterior cruciate ligament tibial avulsion fracture. Knee Surg Sports Traumatol Arthrosc. 2018;26:912-8.
- [CrossRef] [PubMed] [Google Scholar]
- Arthroscopic direct anterior-to-posterior suture suspension fixation for the treatment of posterior cruciate ligament tibial avulsion fracture. Orthop Surg. 2022;14:2031-41.
- [CrossRef] [PubMed] [Google Scholar]
- Arthroscopic suture-to-loop fixation of posterior cruciate ligament tibial avulsion fracture. Arthrosc Tech. 2021;10:e1595-602.
- [CrossRef] [PubMed] [Google Scholar]




