
Translate this page into:
History and evolution of shoulder arthroscopy

*Corresponding author: Sanjay S. Desai, Shoulder and Knee Clinic, 11A Satguru, 16 French Bridge, Mumbai - 400 007, Maharashtra, India. drdesaisanjay@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Desai SS. History and evolution of shoulder arthroscopy. J Arthrosc Surg Sport Med 2020;1(1):11-5.
Abstract
The invention of the incandescent light bulb by Edison in 1879, led to the introduction of the laparo-thoracoscope in 1910. Attempts were made to use this device in the knee joint as well. Development of the arthroscope really took off after the introduction of “cold-light” and rod lens optical system by Hopkins in 1960. Kenji Takagi and later Masaki Watanabe get the credit for developing the modern form of arthroscopy. The spillover of knee arthroscopy into the shoulder was inevitable and began in 1980’s. Shoulder arthroscopy started with instability repair, followed by subacromial decompression. Through the 1980’s and 1990’s, with the development in biotechnology, more sophisticated tools and anchors became available leading to refinement of instability repair procedures. The 2000’s saw improvement in arthroscopic rotator cuff repair techniques including the double- row and trans-osseous equivalent. The last decade has witnessed the development of more complex arthroscopic procedures such as Latarjet and Superior Capsule Reconstruction. However, arthroscopic surgery continues to be equipment intensive and we need to remind ourselves that the arthroscope is no “magic wand” and good clinical evaluation continues to prevail.
Keywords
History
Shoulder
Arthroscopy
Bankart
Rotator cuff

EVOLUTION OF ENDOSCOPY AND DEVELOPMENT OF THE ARTHROSCOPE
The curiosity to look inside has been a natural and insatiable desire of humankind. However, closed cavities had the problem of illumination. Credit for developing the arthroscope goes to certain personalities that had the desire and ability not just to look inside but to look beyond. The first known instrument, “Lichtleiter,” designed to look inside the urinary bladder was presented by Bozini in 1806.[1] Fifty years later, Desormaux developed the “gasogene cystoscope,” which provided light by combustion of gasoline and turpentine that was reflected into the bladder by a mirror.[1] Invention of the incandescent bulb by Edison in 1879 [Figure 1] led to the development of the cystoscope (with an incandescent bulb) in 1886 by Leiter and Nitz in Germany.[2] In 1910, Hans Christian Jacobeaus, from Sweden designed an endoscopic instrument with an incandescent light bulb for use in the abdomen and thorax.[3] It was named “laparo-thoracoscope” [Figure 1]. Severin Nordentoft is considered the first to coin the term arthroscopy in 1912 and used the laparo-thoracoscope in the knee joint.[4] Kenji Takagi from Japan gets the credit of being the first true developer and the father of modern arthroscopy. From 1918 onwards, he continuously worked on the arthroscope, until 1938 when he introduced the 12th design.[5] Simultaneously, in 1921 Swiss surgeon, Eugen Bircher published his work on diagnosis of meniscal pathology using a modified Jacobeaus laparo-thorascope made by Wolf company in Berlin.[6] In 1925 Philip Heinrich Kreuscher from Chicago, published an article entitled “Semilunar Cartilage Disease – A Plea for the Early Recognition by Means of the Arthroscope.”[7] Around 1931 Michel Burman had begun to explore the use of an arthroscope in the anatomy laboratory using a special 4-mm-diameter endoscopic instrument designed for him by Reinhold Wappler, the founder of a fledgling company that later became known as American Cystoscope Makers Inc. The results of his investigations were published in an article entitled “Arthroscopy or the Direct Visualization of Joints.”[8] After the second world war, Masaki Watanabe took over from his mentor Kenji Takagi. Watanabe went onto improvise the arthroscope designed my Takagi and came up with the Watanabe number 21 arthroscope, which became the world’s first production arthroscope [Figure 1].[9] The number 21 was also the world’s last arthroscope with incandescent light bulb, which would often break. Two major innovations changed the game completely, the “cold” light (fiber) and the rod lens optical system, which were introduced by Hopkins [Figure 1] in 1955 and 1960, respectively.[10,11] Finally, in 1967 Watanabe introduced the number 22 arthroscope, which incorporated fiber light (or “cold light”) for illumination, and then in 1970 came the number 25, the first ultrathin fiberoptic endoscope, which had a 2-mm-diameter sheath and a single “selfoc” fiber (1.7 mm in diameter) to transmit the image to the eye. (It later formed the basis of the Dyonics “Needlescope.”) Watanabe was also responsible for introducing the concept of “triangulation.” In 1955, he performed the first recorded operative procedure under arthroscopic control – the removal of a solitary giant cell tumor from a knee joint. Watanabe wrote the first Atlas of arthoscopy in 1957.[12] Japan being the epicenter of arthroscopy, Jackson and Dandy visited Japan and took the technique to Canada, while Richard L O’Connor to North America. Jackson published the first textbook of arthroscopy along with David Dandy.[13] David Dandy then established Arthroscopy in the United Kingdom. The eventual spread of arthroscopy across the globe was inevitable.
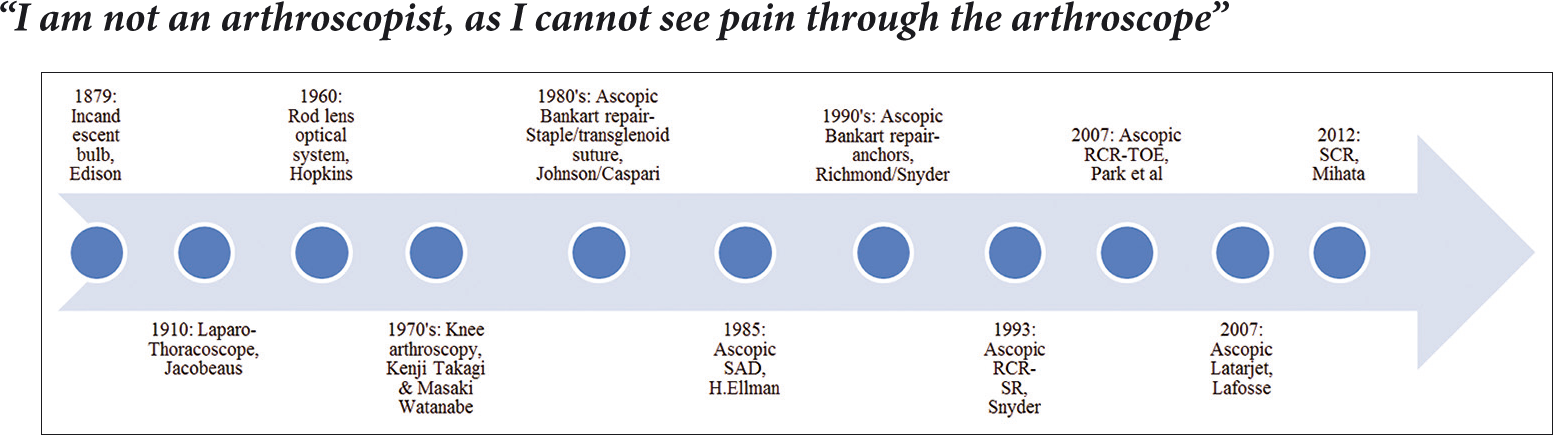
- Timeline of evolution of the arthroscope and important developments in shoulder arthroscopy.
BEGINNING OF SHOULDER ARTHROSCOPY
The 1970’s saw the rise and acceptance of knee arthroscopy as a safe and useful procedure. Its eventual spill over into the shoulder was inevitable. Lanny Johnson was one of the early ones to report on shoulder arthroscopy in 1980.[14]
Mathews et al. described the anterior portal in 1985.[15] It was Eugene Wolfe who came out with need for anterosuperior and anteroinferior portals, for better visualization of the anterior glenoid as well as for better angle of approach for operating on the anteroinferior glenoid.[16] James Tibone in 1995 described the 5’O clock portal, suggesting that it provides an even better angle of approach for instability surgery.[17] In 1988, O’Brien et al. introduced the beach chair position to avoid the brachial plexus strain caused by the lateral position and described its benefit when switching to open surgery.[18]
DEVELOPMENT OF PUMP/RADIOFREQUENCY ABLATOR
The introduction of electrothermal energy was by Aritomi in 1972, for arthroscopic synovectomy.[19] Miller reported the use of electrothermal energy for lateral retinaculum release in 1982.[20] Fox et al. in 1984 further outlined the use of electrosurgery in orthopedics.[21] The idea of using 1.5% glycine as a safe irrigation solution was borrowed from the urologist.[22] Reduced chance of fluid absorption and overload with 1.5% glycine, was reported as a distinct advantage over normal saline and sterile water.[22,23]
Gillquist first described the use of a mechanized pump in arthroscopic surgery in 1977.[24] However, it was Bergstrom form Sweden who described the details of the use of mechanized pump in 1986.[25] Bergstrom said, “The use of an infusion pump is an effective and efficient method of joint irrigation and distention for arthroscopy of the knee. However, the operator cannot forget about the pump. The pump does not think for itself and will continue to automatically place fluid in the joint, regardless of any difficulties it might be causing.”
It is interesting to note that as technology grew, with the development of fluid pumps and electrothermal devices, so did operative procedures started developing across the world of shoulder surgery. We owe a lot to our bioengineers.
ARTHROSCOPIC BANKART REPAIR
Lanny Johnson [Figure 1] was the first to describe arthroscopic stabilization technique in 1980.[14] He used staples, which were difficult to place in the inferior quadrant of the glenoid and resulted in a high failure rate, 16–33%.[14,26,27]
Craig Morgan and Bodenstab introduced the transglenoid suture technique in 1987, later popularized by McIntyre and Caspari.[28,29] There were several modifications of this trans- osseous suture technique. However, the transglenoid suture technique had the disadvantage of the sutures being tied over the infraspinatus fascia, which would eventually become loose leading to high recurrence rate, besides the risk to the suprascapular nerve. Willey showed some promising results with metallic rivets passed through the capsule-labrum which reduced the risk of injury to the suprascapular nerve.[30] The metallic rivets had to be removed after soft-tissue healing; nevertheless, this technique did not gain much popularity. Warner et al. introduced the bio-absorbable tacks in 1995.[31] It had the benefit of not having to remove the implant, however the high incidence of tissue reaction with polyglyconate and the unacceptably high recurrence rate, lead to the natural end of the technique. The use of anchors for arthroscopic Bankart repair was first described by Richmond [Figure 1] in 1991, which was then modified by Wolf in 1993.[32,33] Around same time in 1993, Snyder and Strafford introduced non- absorbable sutures.[34] Anchors provided multiple point fixations and allowed repairing of the capsule-labrum to the edge of the glenoid, thereby reproducing anatomy. This laid the foundation of the technique of arthroscopic Bankart repair as it is done today. Improvements are constantly happening in biomaterials, instrumentation, and anchor design; however, the basic technique of arthroscopic Bankart repair using suture anchors remains fairly standardized and continues to be the most commonly performed procedure for recurrent anterior dislocation of shoulder. The high failure rate of arthroscopic Bankart repair in patients with significant glenoid bone loss as well as those involved in contact sports, led to the development of bone augmentation procedures.[35]
ARTHROSCOPIC BRISTOW-LATARJET PROCEDURE
During the period of WWII, Brigadier Rowley W. Bristow taught the procedure (1940’s) and it was one of his students Helfet (Johannesberg) who published the results in 1958.[36] Michael Latarjet, head of thoracic surgery in Jules-Courmont hospital in Lyon, published his paper on stabilization for traumatic anterior dislocation of shoulder.[37] Interestingly, Trillat described an identical technique in the same edition of the journal.[38] In his description, Latarjet refers to a technique described by Mauclaire, Hybinette, and Eden. Eden, in 1917, transferred a cortico-cancellous bone block from the tibia to the scapular neck to act as an extended buttress of the anterior glenoid.[39] Hybinette described a similar technique using the iliac crest bone graft.[40] The Eden-Hybinette procedure became especially popular in the Scandanavian countries. In 1938, Boicev reported an operation very similar to the one described by Latarjet and Helfet.[41] In this procedure, the coracoid with the attached conjoint tendon is osteotomized and re-routed under the subscapularis to be reached to its original site.[41]
Nourissat was the first to describe a cadaveric study of arthroscopic Bristow-Latarjet procedure.[42] Lafosse [Figure 1] described a detailed technique of arthroscopic Bristow-Latarjet procedure in 2007.[43] In 2016, Boileau described the arthroscopic Bristow-Latarjet technique with suture button fixation of the coracoid.[44] However, due to the high complication rate and a steep learning arthroscopic Bristow-Latarjet remains to be accepted unanimously as a standard procedure by the world.
ARTHROSCOPIC REMPLISSAGE PROCEDURE
In 1972, Conolly had described an open transfer of the infraspinatus and capsule into the Hill-Sachs defect.[45] For large, engaging Hill-Sachs lesion, Eugene Wolf presented (in 2007) a procedure that consists of an arthroscopic posterior capsulodesis and infraspinatus tenodesis to fill (remplissage, which means “to fill” in French) the defect, in addition to an arthroscopic Bankart repair.[46]
ARTHROSCOPIC SUBACROMIAL DECOMPRESSION
Harvard Ellman [Figure 1] first reported arthroscopic subacromial decompression in 1985.[47] He then published a detailed description of the technique, with 1–3 years follow-up in 1987, showing the results are equal to open acromioplasty.[48]
It was one of the most popular arthroscopic shoulder procedures throughout the 1990’s. Eventually, the world realized that the primary source of subacromial impingement is the rotator cuff and not the acromion.
ARTHROSCOPIC ROTATOR CUFF REPAIR
In 1985, Goble was the first to introduce the suture anchor.[49] Following which, the use of the suture anchor for “open” rotator cuff repair started picking up. One of the early reports of arthroscopic rotator cuff repair using suture anchors was by Stephen Snyder [Figure 1] in 1993.[50] However, due to the high re-tear rate, surgeons persevered to improvise the technique to improve the healing rate. Fealy et al., in 2002, reported arthroscopic subacromial decompression and mini-open double-row repair.[51] They said, “We believe that vigorous tendon mobilization combined with a broad surface area to allow for bone-tendon healing provides a suitable environment for repair of rotator cuff tears, including large ones.” Very soon, in same year of 2002 at the 19th Annual San Diego meeting, J. DeBeer presented the “arthroscopic rotator repair by footprint reconstruction,” perhaps the first report of the arthroscopic double-row technique.[52] This was almost immediately followed by the “Double-Row Arthroscopic Rotator Cuff Repair” by Lo and Burkhart in November 2003.[53] The Richard O’Connor award winning study by Apreleva in 2002, demonstrated the three-dimensional rotator footprint and confirmed that single-row repair restored only 67% of the original rotator cuff footprint, whereas trans-osseous simple suture repair restored 85% of the surface area.[54] This finally laid the foundation for the development of the current trans- osseous equivalent technique of arthroscopic rotator cuff repair by Park et al. (California) in 2007 [Figure 1].[55]
AC JOINT/SUPERIOR LABRUM ANTERIOR AND POSTERIOR (SLAP) LESIONS
In 1988, Stephen Snyder described the arthroscopic technique of the well-established open Mumford-Gird procedure.[56] He explained the benefits of not violating the delto-trapezius fascia. He also was the first to report the SLAP lesion and its arthroscopic treatment in 1990.[57] Snyder described, “The injury of the superior labrum begins posteriorly and extends anteriorly, stopping before or at the mid-glenoid notch and including the ‘anchor’ of the biceps tendon to the labrum.” He labeled this injury a “SLAP lesion.” Snyder then used absorbable fixation tack for SLAP-II repair.
ARTHROSCOPIC SUPERIOR CAPSULE RECONSTRUCTION (SCR)
In 2007, it was perhaps the unavailability of reverse shoulder prosthesis in Japan that drove Teruhisa Mihata [Figure 1] to use Fascia Lata for SCR in patients with massive irreparable rotator cuff tears.[58] The need to harvest the Fascia Lata led to the application of synthetic patch for irreparable massive rotator cuff tears, using the same principles of SCR. The acellular dermal matrix allograft, GraftJacket, was introduced by Wright Medical in 2003.[59] Snyder first reported the early results of the GraftJacket for massive irreparable rotator cuff tear in 2008.[60] The management of massive irreparable rotator cuff tear in young remains a challenge, while the principles and technique of SCR continue to evolve.
Declaration of patient consent
Patient’s consent not required as there are no patients in this study.
Financial support and sponsorship
Nil.
Conflicts of interest
Dr. Sanjay S. Desai is on the Editorial Board of the Journal.
References
- Catalogue Prepared by the Staff of the National Museum for the History of Science. Leiden.
- The Electric Illumination of the Bladder and Urethra London: J and A Churchill; 1889.
- [Google Scholar]
- Endoscopy of closed cavities using my trokart endoscope. Verh Dtsch Ges Chir. 1912;1912:78-81.
- [Google Scholar]
- Semilunar cartilage disease-a plea for the early recognition by means of the arthroscope. Ill Med J. 1925;47:290-2.
- [Google Scholar]
- Arthroscopy or the direct visualization of joints: An experimental cadaver study. J Bone Joint Surg. 1931;13:669-95.
- [Google Scholar]
- Transparent fibres for the transmission of optical images. Opt Acta. 1955;1:164-70.
- [CrossRef] [Google Scholar]
- Improvements in or Relating to Optical Systems United Kingdom: British Patent; 1960.
- [Google Scholar]
- Tokyo: Atlas of Arthroscopy. Igaku Shoin Ltd.;
- Anterior portal selection for shoulder arthroscopy. Arthroscopy. 1985;1:33-9.
- [CrossRef] [Google Scholar]
- Anterior-inferior (5 O'clock) portal for shoulder arthroscopy. Arthroscopy. 1995;11:519-25.
- [CrossRef] [Google Scholar]
- Shoulder arthroscopy with the patient in the beach-chair position. Arthroscopy. 1988;4:256-9.
- [CrossRef] [Google Scholar]
- A method of arthroscopic surgery. Clinical evaluation of synovectomy with the electric resectoscope and removal of loose bodies in the knee joint. Orthop Clin North Am. 1979;10:565-84.
- [Google Scholar]
- The use of electrosurgery for arthroscopic subcutaneous lateral release. Orthopedics. 1982;5:309-14.
- [Google Scholar]
- Determination of absorption of irrigating fluid during transurethral resection of the prostate by means of radioisotopes. J Urol. 1969;102:714-9.
- [CrossRef] [Google Scholar]
- Observations in cardiac output, blood volume, central venous pressure, fluid and electrolyte changes in patients undergoing transurethral prostatectomy. J Urol. 1970;103:632-6.
- [CrossRef] [Google Scholar]
- Arthroscopy in acute injuries of the knee joint. Acta Orthop Scand. 1977;48:190-6.
- [CrossRef] [PubMed] [Google Scholar]
- Complications about the glenohumeral joint related to the use of screws and staples. J Bone Joint Surg Am. 1984;66:175-80.
- [CrossRef] [Google Scholar]
- Arthroscopic stapling repair for shoulder instability: A retrospective study of 50 cases. Arthroscopy. 1989;5:122-8.
- [CrossRef] [Google Scholar]
- Arthroscopic Bankart suture repair: Technique and early results. Arthroscopy. 1987;3:111-22.
- [CrossRef] [Google Scholar]
- Arthroscopic reconstruction for anterior shoulder instability. Tech Orthop. 1988;3:59-66.
- [CrossRef] [Google Scholar]
- Arthroscopy for shoulder instability and a technique for arthroscopic repair. Arthroscopy. 1988;4:25-30.
- [CrossRef] [Google Scholar]
- Arthroscopic Bankart repair with the suretac device. Part II: Experimental observations. Arthroscopy. 1995;11:14-20.
- [CrossRef] [Google Scholar]
- Arthroscopic Bankart repair using suture anchors. Oper Tech Orthop. 1991;1:194.
- [CrossRef] [Google Scholar]
- Arthroscopic capsulolabral repair using suture anchors. Orthop Clin North Am. 1993;24:59-69.
- [Google Scholar]
- Arthroscopic management of instability of the shoulder. Orthopedics. 1993;16:993-1002.
- [Google Scholar]
- Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: Significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy. 2000;16:677-94.
- [CrossRef] [PubMed] [Google Scholar]
- Coracoid transplantation for recurring dislocation of the shoulder. J Bone Joint Surg Br. 1958;40:198-202.
- [CrossRef] [PubMed] [Google Scholar]
- Technic of coracoid preglenoid arthroereisis in the treatment of recurrent dislocation of the shoulder. Lyon Chir. 1958;54:604-7.
- [Google Scholar]
- Treatment of recurrent dislocation of the shoulder; technical considerations. Lyon Chir. 1954;49:986-93.
- [Google Scholar]
- For the operation of habitual shoulder dislocation undernotification of a new procedure in the event of a tear on the inside pan edge. Dtsch Z Chir. 1918;144:268-80.
- [Google Scholar]
- Transplanting a bone fragment for remedy of recurrent dislocations of the shoulder; findings and operational results. Acta Orthop Scand. 1932;71:411-45.
- [Google Scholar]
- Mini-open arthroscopically assisted Bristow-Latarjet procedure for the treatment of patients with anterior shoulder instability: A cadaver study. Arthroscopy. 2006;22:1113-8.
- [CrossRef] [PubMed] [Google Scholar]
- The arthroscopic Latarjet procedure for the treatment of anterior shoulder instability. Arthroscopy. 2007;23:1242-5.
- [CrossRef] [PubMed] [Google Scholar]
- A guided surgical approach and novel fixation method for arthroscopic Latarjet. J Shoulder Elbow Surg. 2016;25:78-89.
- [CrossRef] [PubMed] [Google Scholar]
- Humeral head defects associated with shoulder dislocation: Their diagnostic and surgical significance. Instr Course Lect. 1972;21:42-54.
- [Google Scholar]
- Hill-Sachs remplissage: An arthroscopic solution for the engaging Hill-Sachs lesion. Arthroscopy. 2004;20:e14-5.
- [CrossRef] [Google Scholar]
- Arthroscopic subacromial decompression: Analysis of one to three year results. Arthroscopy. 1987;3:173-81.
- [CrossRef] [Google Scholar]
- The development of suture anchors for use in soft tissue fixation to bone. Am J Sports Med. 1994;22:236-9.
- [CrossRef] [PubMed] [Google Scholar]
- Arthroscopic fixation of rotator cuff tears with multiple screw anchors In: Proceedings of the Annual Meet Ing of the American Shoulder and Elbow Surgeons. Virginia, Williamsburg: American Shoulder and Elbow Surgeons; 1993.
- [Google Scholar]
- Mini-open rotator cuff repair using a two-row fixation technique: Outcomes analysis in patients with small, moderate, and large rotator cuff tears. Arthroscopy. 2002;18:665-70.
- [CrossRef] [PubMed] [Google Scholar]
- Double-row arthroscopic rotator cuff-repair: Re-establishing the footprint of the rotator cuff. Arthroscopy. 2003;19:1035-42.
- [CrossRef] [PubMed] [Google Scholar]
- Rotator cuff tears: The effect of the reconstruction method on three-dimensional repair site area. Arthroscopy. 2001;18:519.
- [CrossRef] [PubMed] [Google Scholar]
- Part I: Footprint contact characteristics for a transosseous-equivalent rotator cuff repair technique compared with a double-row repair technique. J Shoulder Elbow Surg. 2007;16:461-8.
- [CrossRef] [Google Scholar]
- Arthroscopic acromioclavicular joint debridement and distal clavicle resection. Orthop Tech. 1988;3:41-45.
- [CrossRef] [Google Scholar]
- Superior capsule reconstruction to restore superior stability in irreparable rotator cuff tears: A biomechanical cadaveric study. Am J Sports Med. 2012;40:2248-55.
- [CrossRef] [PubMed] [Google Scholar]
- Graft Jacket Rotator Cuff Tendon Reinforcement Scaffold-Surgical Techniques Arlington, Tennessee: Wright Medical Technology, Inc.; 2003.
- [Google Scholar]
- Arthroscopic replacement of massive, irreparable rotator cuff tears using a graftjacket allograft: Technique and preliminary results. Arthroscopy. 2008;24:403-9.
- [CrossRef] [PubMed] [Google Scholar]




