
Translate this page into:
Inside-out repair of complex tears in the posterior horn of the lateral meniscus
*Corresponding author: I. Geethan, Department of Orthopedics, Dhanalakshmi Srinivasan Medical College, Siruvachur, Perambalur, Tamil Nadu, India igeethan@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Geethan I. Inside-out repair of complex tears in the posterior horn of the lateral meniscus. J Arthrosc Surg Sports Med. 2024;5:59-61. doi: 10.25259/JASSM_32_2022
Abstract
All-inside meniscus devices are preferred over inside-out sutures for complex tears in the posterior horn of the lateral meniscus due to the ease of use, avoidance of additional skin incisions, and reduced surgical time. However, inside-out sutures have the advantages of being less traumatic due to smaller diameter needles, better healing rate, and less chance of injuries to posterior neurovascular structures due to direct visualization and protection. To the author’s knowledge, the inside-out repair technique has been described only for vertical tears and not for complex tears in the posterior horn of the lateral meniscus. This video describes the technique of repairing complex lateral meniscus tears with inside-out sutures using various suture configurations. The lateral meniscus tear pattern is identified. A posterolateral safety incision is made, and a retractor is placed posterior to the capsule. The popliteal vein is identified at this step and kept under visualization to avoid injury. Meniscal repair configurations such as “H,” “X,” and “A” patterns and simple vertical or horizontal sutures are planned according to the tear pattern. Sutures are passed using inside-out meniscal sutures, 18G spinal needle, self-retrieving suture devices or a combination of those, and tied over the capsule using sliding knots while the repair site is arthroscopically visualized.
Keywords
Lateral meniscus
Lateral meniscus repair
Inside-out repair
Posterolateral safety incision

INTRODUCTION
Lateral meniscus tears are frequently seen in association with anterior cruciate ligament injuries. Compared to the medial meniscus, lateral meniscectomy has a poorer outcome.[1] Lateral meniscectomy increases the joint reaction forces by about 200–300% compared to medial meniscectomy, which increases the joint reaction force by about 100%.[2] Fortunately, lateral meniscus repair has a better healing rate.[3] All-inside repair using implants is the preferred method for repairing tears in the posterior horn of the lateral meniscus. However, inside-out sutures have the advantages of being less traumatic due to smaller diameter needles, better healing rate,[4] and less chance of injuries to posterior neurovascular structures due to direct visualization and protection. To the author’s knowledge, the inside-out repair technique has been described only for vertical tears and not for complex tears in the posterior horn of the lateral meniscus. This video describes the technique of repairing complex lateral meniscus tears with inside-out sutures using various suture configurations.
SURGICAL TECHNIQUE
An arthroscopic examination of the knee joint is performed, and concomitant lesions are addressed. The lateral meniscus tear pattern is identified and assessed regarding its reducibility. Only those tears in the red-red or red-white zones and reducible without tension are chosen for repair. The knee is kept at 90° flexion. A 5-centimeter-long posterolateral safety incision is made along a line extending from the posterior border of the fibula. The incision is made with two-fifths of its length above and three-fifths below the joint line [Figure 1]. The fascia lata and the biceps femoris muscle are identified by the tendinous strands of the fascia lata and muscular strands of the biceps femoris [Figure 2]. Superficial dissection is between the biceps femoris tendon and fascia lata [Figure 3]. Deep dissection is between the lateral head of the gastrocnemius and the capsule [Figure 4]. The dissection is extended to the midline to visualize the popliteal vein [Figure 5]. The popliteal artery is medial to the vein, and the posterior tibial nerve is superficial to be vein. Both structures are away from the dissection performed from the lateral side. Visualization and protection of the popliteal vein protects the nerve and artery. A popliteal retractor is placed in the wound, and it protects the common peroneal nerve. The knee is placed in a figure-of-four position, with the hip externally rotated and the knee in 70-90° of flexion. The lateral meniscus tear is visualized under arthroscopic guidance, reduced, and multiple inside-out sutures are passed and retrieved through the posterolateral safety incision. The sutures are passed with the knee in the figure-of-four position, and the arthroscope is placed in the posterolateral safety incision to visualize and retrieve the sutures. The technique is described in Video 1.
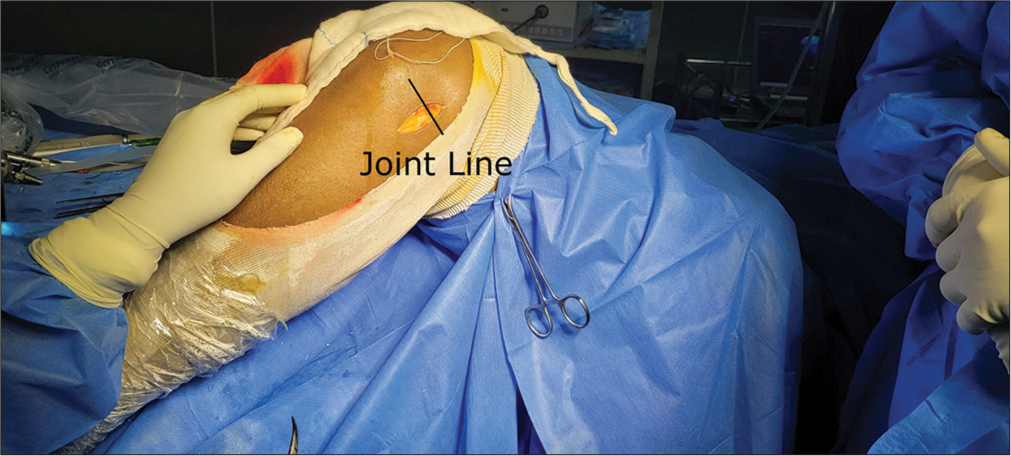
- Skin incision.
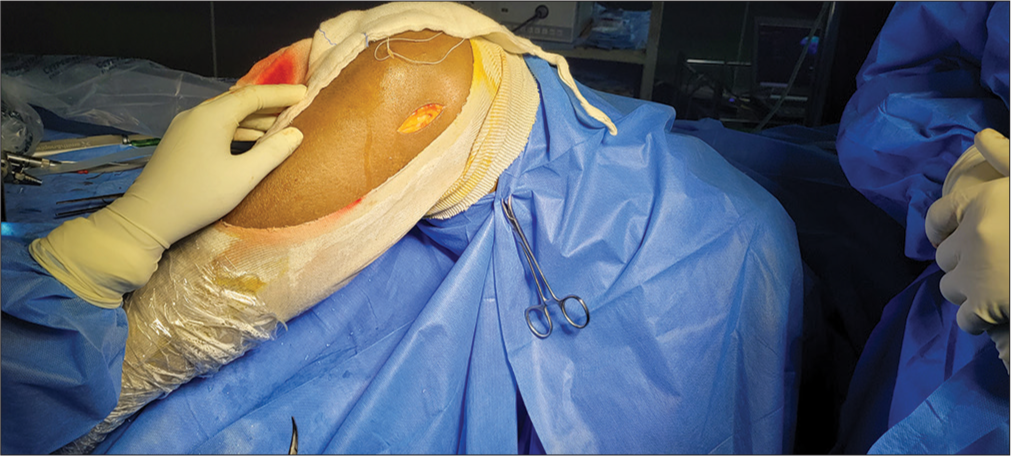
- Identification of fascia lata (tendinous, white-yellow color) and biceps femoris (muscular, brown color).
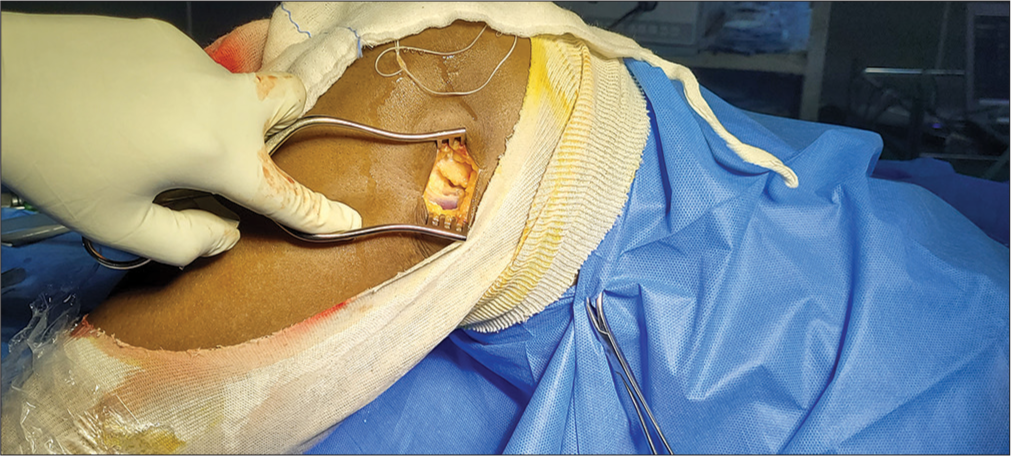
- Superficial dissection.
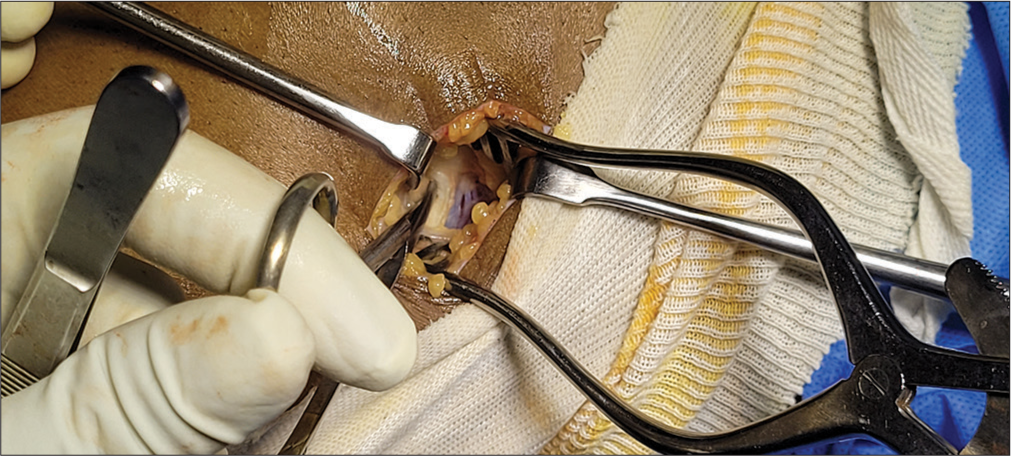
- Deep dissection.
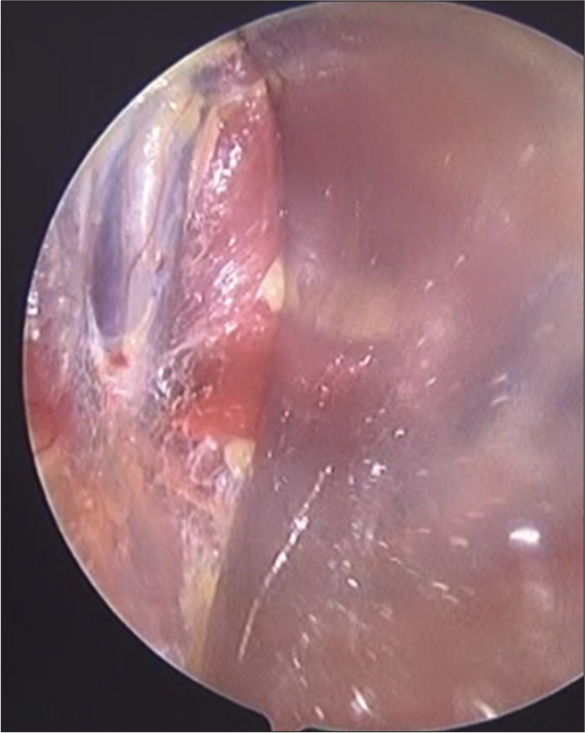
- Identification of popliteal vein.
Video 1:
Video 1:Technique video demonstrating the inside-out repair of the tears in the posterior horn of the lateral meniscus.DISCUSSION
The concerns in meniscal repair are the potential for healing and the risk of injury to neurovascular structures. While the lateral meniscus has good healing potential, inside-out repair of the lateral meniscus is complicated by the presence of popliteal tendon and neurovascular structures. All-inside lateral meniscal repair from either the medial or lateral portal has the risk of iatrogenic neurovascular injury.[5] We propose the visualization of the popliteal vein through the posterolateral safety incision as a landmark to prevent iatrogenic injury. Anatomical studies have shown that the popliteal vein is the most deep-lateral structure among the neurovascular structures. The visualization of the popliteal vein will protect the popliteal artery, which lies farther (medial) and the posterior tibial nerve, which lies posterior. The popliteal retractor protects the common peroneal nerve. The use of antegrade suture passing-retrieving devices such as Meniscal Scorpion (Arthrex, Naples, Florida, USA) and FastPass Mini (Smith and Nephew, London, UK) has extended the indication of inside-out repairs for complex tears of the posterior horn of the lateral meniscus. While these devices can be used for placing sutures and intraarticular knots, in certain cases, such as poor meniscal tissue quality and small meniscal fragments, extracapsular knots may offer secure fixation. Antegrade sutures are placed in the flap portion of the tear, and the suture limbs are retrieved and tied posterior to the capsule through a posterolateral safety incision. The use of smaller diameter needles and the lesser cost of the procedure are added advantages of inside-out repair. The disadvantages of this technique include increased operative time, risks of needle stick injuries, and the need for adequate training to perform this procedure.
CONCLUSION
The inside-out repair technique is a viable option for repairing meniscal tears in the posterior horn of the lateral meniscus. This method offers several advantages, including minimal meniscal tissue injury due to the use of smaller diameter needles and reduced procedure costs. In addition, visualizing the popliteal vein helps in reducing the risk of neurovascular damage. However, more comparative trials with a larger number of cases are necessary to determine if the risk of neurovascular injuries is lower when using this technique.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Return to play after lateral meniscectomy compared with medial meniscectomy in elite professional soccer players. Am J Sports Med. 2014;42:2193-8.
- [CrossRef] [PubMed] [Google Scholar]
- Meniscal tears: The effect of meniscectomy and of repair on intraarticular contact areas and stress in the human knee. A preliminary report. Am J Sports Med. 1986;14:270-5.
- [CrossRef] [PubMed] [Google Scholar]
- Meniscal repair in the elite athlete: Results of 45 repairs with a minimum 5-year follow-up. Am J Sports Med. 2009;37:1131-4.
- [CrossRef] [PubMed] [Google Scholar]
- Inside-out medial meniscal repair: Improved surgical exposure with a sub-semimembranosus approach. Arthrosc Tech. 2021;10:e507-17.
- [CrossRef] [PubMed] [Google Scholar]
- The danger zone for iatrogenic neurovascular injury in all-inside lateral meniscal repair in relation to the popliteal tendon: An MRI study. Orthop J Sports Med 2021 Doi: 10.1177/23259671211038397
- [CrossRef] [PubMed] [Google Scholar]




