
Translate this page into:
Relation of arthroscopic measurement of tibial footprint with the height, weight, or gender of patients: A pilot study on Indian subject

*Corresponding author: Bibhuti Nath Mishra, Department of Orthopaedics, Joint and Bone Care Hospital, Salt Lake City, Kolkata, West Bengal, India. drbibhuti5@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Mishra BN, Raman R, Patowary S, Longkeng CM. Relation of arthroscopic measurement of tibial footprint with the height, weight, or gender of patients: A pilot study on Indian subject. J Arthrosc Surg Sports Med 2021;2(1):13-7.
Abstract
Objectives:
A prospective study performed to evaluate whether any correlation exists between tibial footprint size (length and width) of anterior cruciate ligament (ACL) with the height, weight, or gender of patients.
Materials and Methods:
A total of 53 patients presenting with an ACL tear (54 knees) in 8 months duration who underwent ACL reconstruction were evaluated for height, weight, and gender. Arthroscopic measurement of ACL footprint’s length and width with calibrated probe and measuring scale was done and the average of those measurements was recorded and compared using SPSS software.
Results:
Out of 53 Patients, 45 were male with a mean age of 28.73 years and a mean height of 66.67 inches. Their mean ACL footprint dimension was 17.40 mm × 7.67 mm2. The remaining eight were female patients with a mean age of 29.2 years and a mean height of 66.17 inches. Their mean ACL footprint dimension was 17.35 mm × 7.61 mm2. Correlation between ACL tibia footprint length versus width was found to be statistically significant. However, the correlation between the patient’s height or weight versus ACL tibial footprint (length and width) was not significant statistically.
Conclusion:
ACL footprint size cannot be predicted from the height, weight, or gender of patients.
Keywords
Height
Weight
Gender
Footprint
Anterior cruciate ligament
Arthroscopy

INTRODUCTION
The anteromedial (AM) and posterolateral (PL) bundles of anterior cruciate ligament (ACL) strongly suggest that ACL is a double-bundle (DB) structure rather being homogenous single bundle (SB).[1-3] After the arthroscopic reconstruction of ACL started, SB ACL reconstruction has been widely practiced. But recently, people thought that with SB ACL reconstruction, the biomechanical and anatomical properties of its native PL bundle are not considered enough in comparison to its native ACL.[4-7] Hence, the DB ACL reconstruction came up considering that it would closely mimic the anatomical and functional properties of native ACL.[8] Few biomechanical studies even showed that the PL bundle reconstruction in DB-ACL reconstruction provides more anterior as well as rotational stability.[9-11] But still, no controlled clinical trials have established the superiority of DB over SB ACL reconstruction.[12,13] Therefore, a detailed knowledge of the size and shape of the tibial footprints of the 2 ACL bundles is of great importance.
We could not find any study suggesting a parameter for ACL footprint size prediction preoperatively.[12,13] In case, we get one of such predictors, the pre-operative planning and patient counseling would become far easier. Thus, this study aims to evaluate whether any correlation exists between tibial footprint size (length and width) of ACL with the height, weight, or gender of patients.
MATERIALS AND METHODS
This is a prospective study conducted in 10 months’ duration (February 2019–November 2019). All cases were operated by single surgeon at one center. All ACL tears with or without meniscus tear presenting in specified study duration were included in this study. The multiligament injuries and ACL tears with associated posterior cruciate ligament tears were excluded. Details of ongoing study were explained to all patients and written consent was received from each of them. Pre-evaluation and documentation of height, weight, and gender of patients were done. Arthroscopic debridement of ACL tibial footprint base was done during the procedure and tibial footprint’s length and width were measured with calibrated probe and measuring scale separately [Figure 1]. Average of those measurements was recorded. The bivariate regression analysis using SPSS software was used for statistical analysis.
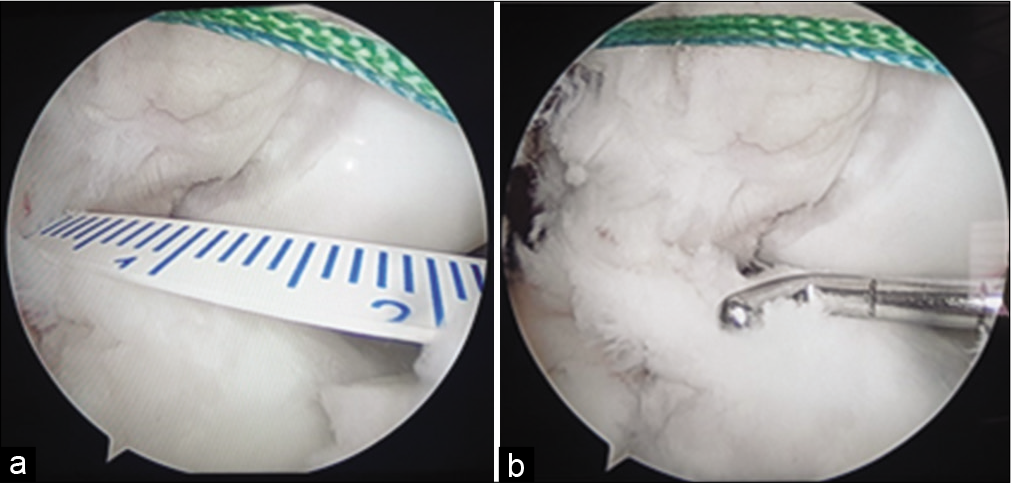
- Anterior cruciate ligament tibial footprint base measured with calibrated probe (a) and measuring scale (b).
RESULTS
A total of 54 knees in 53 patients were included (one bilateral ACL injury). There were 46 males and 8 females [Figure 2] and more right knees in comparison to left [Figure 3].
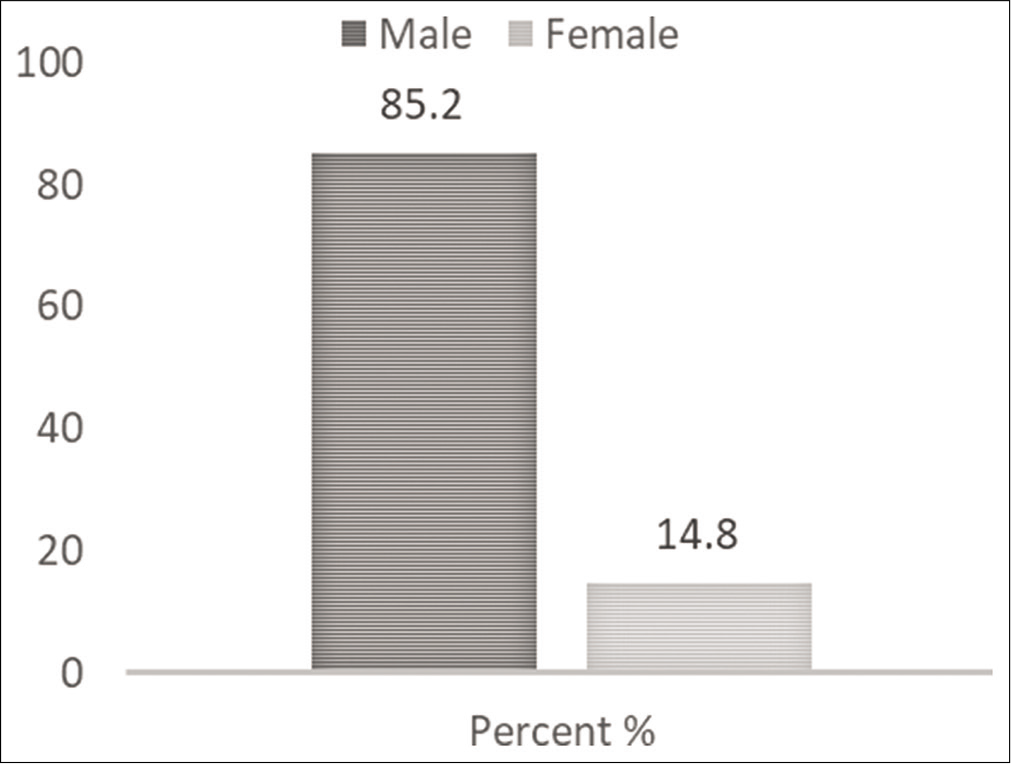
- Gender ratio of patients.
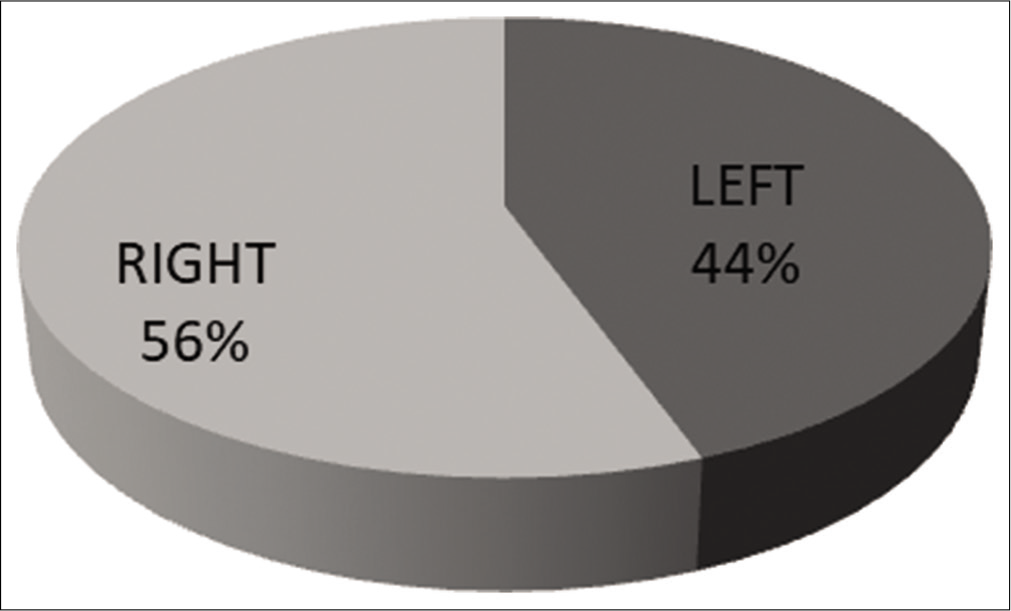
- Frequency of right versus left knees.
The mean age of patients was 29.20 years with mean height of 66.17 inches and the mean ACL footprint dimension of 17.35 mm2 × 7.61 mm2 [Table 1]. Looking gender wise, the values were quite closer in males and females. The t-test and P-values for gender versus ACL length and width were not significant statistically [Table 2].
| Descriptive statistics | n | Minimum | Maximum | Mean | SD |
|---|---|---|---|---|---|
| Age (years) | 54 | 15 | 50 | 29.20 | 9.708 |
| Height (inch) | 54 | 60 | 71 | 66.17 | 2.478 |
| ACL footprint length (mm) | 54 | 10 | 20 | 17.35 | 2.258 |
| ACL footprint width (mm) | 54 | 6 | 10 | 7.61 | 0.811 |
| Valid N (list wise) | 54 |
ACL: Anterior cruciate ligament
| Mean | ||||
|---|---|---|---|---|
| Male | Female | t-value | P-value | |
| Age (years) | 28.73 | 33.88 | ||
| Height (inch) | 66.67 | 63.25 | ||
| ACL footprint length (mm)* | 17.40 | 17.00 | 0.45409 | 0.325845* |
| ACL footprint width (mm)* | 7.67 | 7.38 | 0.93271 | 0.177683* |
*The result is not significant at P<0.05 for genders versus ACL dimension. ACL: Anterior cruciate ligament
Correlation between ACL tibia footprint length versus width was found to be statistically significant. However, the correlation between patient’s height versus ACL tibial footprint (length and width) was not significant statistically [Table 3 and Figure 4]. Similarly, the correlation between patient’s weight versus ACL tibial footprint [length and width] was not significant statistically as well [Table 4].
| Correlations | |||
|---|---|---|---|
| Height (inch) | ACL footprint length (mm) | ACL footprint width (mm) | |
| Height (inch) | |||
| Pearson correlation | 1 | 0.215 | 0.202 |
| Sig. (two tailed) | 0.118* | 0.143* | |
| n | 54 | 54 | 54 |
| ACL footprint length (mm) | |||
| Pearson’s correlation | 0.215 | 1 | 0.530** |
| Sig. (two tailed) | 0.118* | 0.000 | |
| n | 54 | 54 | 54 |
| ACL footprint width (mm) | |||
| Pearson’s correlation | 0.202 | 0.530** | 1 |
| Sig. (two tailed) | 0.143* | 0.000 | |
| n | 54 | 54 | 54 |
**Correlation is significant at the 0.01 level (two tailed). ACL: Anterior cruciate ligament
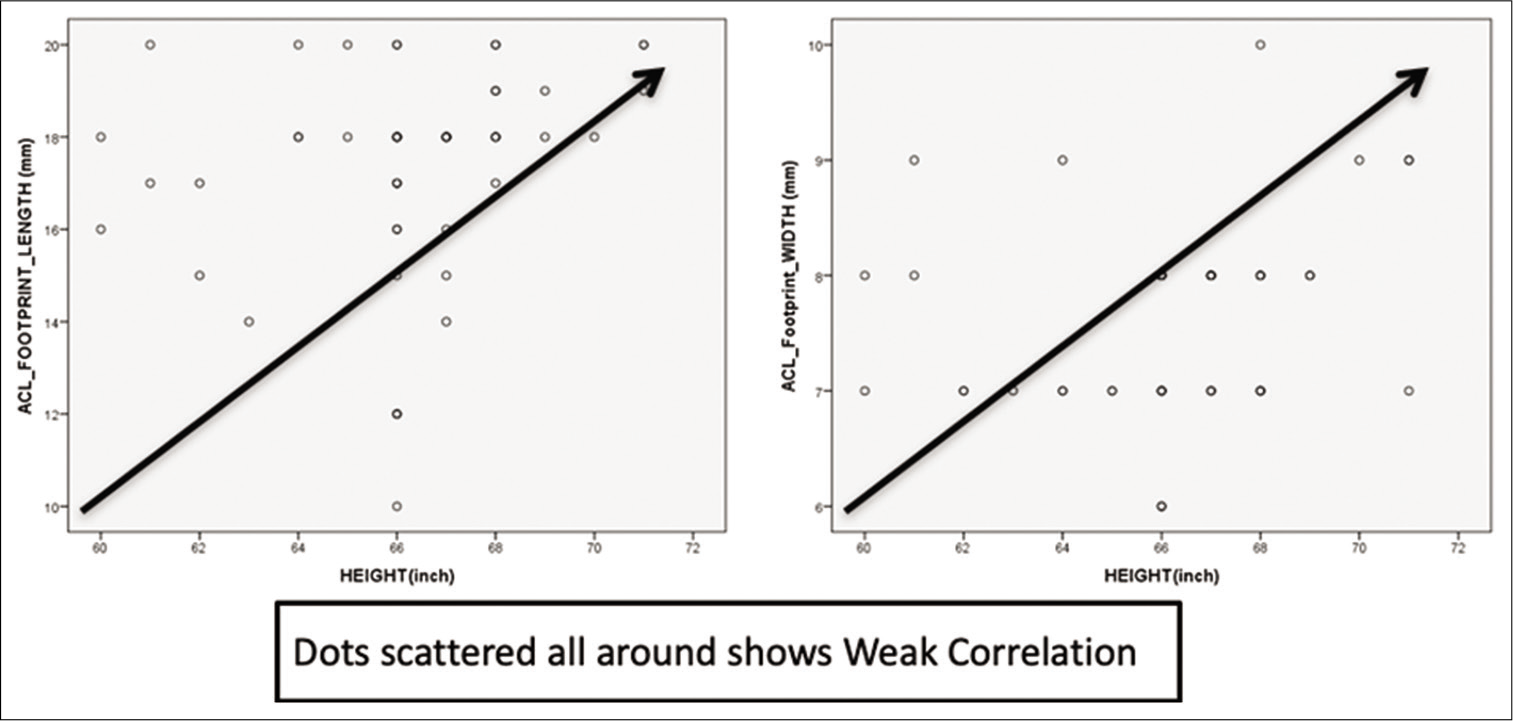
- Correlation of patient’s height versus anterior cruciate ligament tibial footprint.
| Correlations | |||
|---|---|---|---|
| Weight (kg) | ACL footprint length (mm) | ACL footprint width (mm) | |
| Weight (kg) | |||
| Pearson correlation | 1 | 0.226 | 0.332* |
| Sig. (two tailed) | 0.100 | 0.014 | |
| n | 54 | 54 | 54 |
| ACL footprint length (mm) | |||
| Pearson’s correlation | 0.226 | 1 | 0.530** |
| Sig. (two tailed) | 0.100 | 0.000 | |
| n | 54 | 54 | 54 |
| ACL footprint width (mm) | |||
| Pearson’s correlation | 0.332* | 0.530** | 1 |
| Sig. (two tailed) | 0.014 | 0.000 | |
| n | 54 | 54 | 54 |
DISCUSSION
With advancements in sports activities and increased rush in traffic, ACL injuries have become more common.[12] Simultaneously, with the advancements in ligament reconstructions and arthroscopic surgeries, surgeons are focusing on precision, accuracy, and anatomical reconstruction of ACL. People started with trans-tibial non-anatomic ACL reconstruction, switched to trans-portal anatomic ACL reconstructions, and now, huge debate is going on whether SB ACL reconstruction or DB ACL reconstruction. Girgis et al. showed that the two functional bundles of ACL retain different tension properties in flexion and extension of knee, the AM bundle fibers are taught in flexion, and the entire ligament is taught in extension.[14] Norwood and Cross illustrated that it is the AM bundle which resists anterior translation of tibia, whereas the rotatory stability of knee is controlled by PL bundle.[15] Roles of two functional bundles for knee kinematics restoration have been explained by many biomechanical studies[16-18] and thus many studies these days recommend DB ACL reconstruction.[12]
However, when we talk about accuracy or precision of ACLR, the anatomy of its femoral and tibial footprints should be understood properly. There are few studies on anatomic correlation of femoral footprint of ACL and those studies fail to establish strong correlation of height or gender with ACL footprint size.[12,19] A cadaveric knee study on tibial footprint of ACL has attempted to describe the morphometric and topographic anatomy of tibial insertion of AM and PL bundles of ACL but even this study could not show that age or any other parameter has impact on ACL insertion size.[2] Good studies could not be found suggesting any parameter for pre-operative prediction of ACL footprint size.[12,13]
Our study attempts to see whether height or weight of patient has any correlation with ACL footprint’s size. Correlation between ACL tibia footprint’s length versus width was found to be statistically significant in males, females, and overall. However, the correlation between patient’s height versus ACL tibial footprint (length and width) was not significant statistically in males, females, or overall. Strong correlation could not be seen between tibial footprint diameter of ACL with height or weight of patients. Hence, ACL footprint size cannot be predicted from height or weight of patient and we also recommend to measure the ACL tibial footprint size in every case for bone tunnel placement in DB-ACLR.
However, this study has certain limitations. Small sample size and observer biasness are few of them as only approximate and not exact measurement can be done arthroscopically. Many studies are available in literature on Western patients as subjects where femoral/tibial length, width, condylar width, notch width, and many more clinical and radiologic parameters are studied to correlate with ACL footprint dimensions,[12,19,20] but those studies are either cadaveric, radiological, or clinical studies with open technique measurements (mostly during knee replacements). However, our study is done with pure arthroscopic technique, so we did not perform other measurements like condylar/notch width due to technical difficulties to do it arthroscopically.
CONCLUSION
No statistically significant correlation was found between tibial footprint diameter of ACL with height, weight, or gender of patients. However, the coefficient correlation remained weakly positive in male, female, and overall. Hence, ACL footprint size cannot be predicted from gender, height, or weight of patients.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
Dr. Rajeev Raman is on the Editorial Board of the Journal.
References
- Morphology of anterior cruciate ligament attachments for anatomic reconstruction: A cadaveric dissection and radiographic study. Arthroscopy. 2006;22:984-92.
- [CrossRef] [PubMed] [Google Scholar]
- Tibial insertions of the anteromedial and posterolateral bundles of the anterior cruciate ligament: Morphometry, arthroscopic landmarks, and orientation model for bone tunnel placement. Arthroscopy. 2008;24:154-61.
- [CrossRef] [PubMed] [Google Scholar]
- Quantitative analysis of human cruciate ligament insertions. Arthroscopy. 1999;15:741-9.
- [CrossRef] [Google Scholar]
- Anatomic double-bundle anterior cruciate ligament reconstruction. Arthroscopy. 2006;22:1000-6.
- [CrossRef] [PubMed] [Google Scholar]
- Current trends in anterior cruciate ligament reconstruction: Part II. Operative procedures and clinical correlations. Am J Sports Med. 2000;28:124-30.
- [CrossRef] [PubMed] [Google Scholar]
- Excessive tibial rotation during high-demand activities is not restored by anterior cruciate ligament reconstruction. Arthroscopy. 2005;21:1323-9.
- [CrossRef] [PubMed] [Google Scholar]
- In situ forces in the anterior cruciate ligament and its bundles in response to anterior tibial loads. J Orthop Res. 1997;15:285-93.
- [CrossRef] [PubMed] [Google Scholar]
- Double-stranded hamstring graft for anterior cruciate ligament reconstruction. Arthroscopy. 2004;20:890-4.
- [CrossRef] [Google Scholar]
- Strain inhomogeneity in the anterior cruciate ligament under application of external and muscular loads. J Biomech Eng. 1998;120:497-503.
- [CrossRef] [PubMed] [Google Scholar]
- The interrelation of fiber bundles in the anterior cruciate ligament. J Orthop Res. 1990;8:180-8.
- [CrossRef] [PubMed] [Google Scholar]
- Direct measurement of strain in the posterolateral bundle of the anterior cruciate ligament. J Biomech. 1997;30:281-3.
- [CrossRef] [Google Scholar]
- No correlation of height or gender with anterior cruciate ligament footprint size. J Knee Surg. 2011;24:39-44.
- [CrossRef] [PubMed] [Google Scholar]
- Anatomic double-bundle anterior cruciate ligament reconstruction: Where are we today? Arthroscopy. 2008;24:1168-77.
- [CrossRef] [PubMed] [Google Scholar]
- The cruciate ligaments of the knee joint. Anatomical, functional and experimental analysis. Clin Orthop Relat Res. 1975;106:216-31.
- [CrossRef] [PubMed] [Google Scholar]
- The intercondylar shelf and the anterior cruciate ligament. Am J Sports Med. 1977;5:171-6.
- [CrossRef] [PubMed] [Google Scholar]
- Single-versus two-femoral socket anterior cruciate ligament reconstruction technique: Biomechanical analysis using a robotic simulator. Arthroscopy. 2001;17:708-16.
- [CrossRef] [PubMed] [Google Scholar]
- Tunnel positioning of anteromedial and posterolateral bundles in anatomic anterior cruciate ligament reconstruction: Anatomic and radiographic findings. Am J Sports Med. 2008;36:65-72.
- [CrossRef] [PubMed] [Google Scholar]
- Biomechanical analysis of an anatomic anterior cruciate ligament reconstruction. Am J Sports Med. 2002;30:660-6.
- [CrossRef] [PubMed] [Google Scholar]
- Sex-Based differences in the anthropometric characteristics of the anterior cruciate ligament and its relation to intercondylar notch geometry: A cadaveric study. Am J Sports Med. 2005;33:1492-8.
- [CrossRef] [PubMed] [Google Scholar]
- Correlation of anthropometric measurements, strength, anterior cruciate ligament size, and intercondylar notch characteristics to sex differences in anterior cruciate ligament tear rates. Am J Sports Med. 2001;29:58-66.
- [CrossRef] [PubMed] [Google Scholar]




