
Translate this page into:
Outside-in drilling of femoral tunnel in primary anterior cruciate ligament reconstruction made easy and reproducible

*Corresponding author: Raju Easwaran, Shree Meenakshi Orthopedics and Sports Medicine Clinc, B H 41 East Shalimar Bagh, New Delhi, India. contact@drraju.in
-
Received: ,
Accepted: ,
How to cite this article: Easwaran R. Outside-in drilling of femoral tunnel in primary anterior cruciate ligament reconstruction made easy and reproducible. J Arthrosc Surg Sports Med 2021;2(2):131-4.
Abstract
This paper describes a simple, reproducible technique of placing the femoral guide wire perfectly in primary/ revision anterior cruciate ligament reconstruction using a bull’s eye outside-in jig. Technique pearls and pitfalls are also mentioned.
Keywords
ACL reconstruction
Outside-in femoral drilling
Anatomic ACL reconstruction

INTRODUCTION
It is commonly assumed that outside-in drilling of the femoral tunnel in anterior cruciate ligament reconstruction (ACLR) is as easy and convenient as an outside-in drilled femoral tunnel for posterior cruciate ligament reconstruction (PCLR). Outside in femoral tunnel drilling in ACLR offers several advantages, like the ability to drill with the knee in 90 degree flexion.[1] The only disadvantage is the need to give an additional lateral incision.[2] This can easily be converted into an advantage by extending it and utilizing it for harvesting a strip of Ilio-Tibial Band (ITB) in case, an lateral extra-articular tenodesis (LET) is also planned. The common indications therefore to consider outside in femoral drilling in ACL reconstruction are as follows:
When a multi-ligament injury is being operated on to prevent tunnel coalescence with the lateral collateral and popliteal tunnels
In a primary ACLR for high demand patients or where the hamstring graft is expected to be inadequate (short statured/obese), ipsilateral Central Quadriceps Tendon (CQT) with patellar bone plug and Bone Tendon Bone (BTB) grafts are preferred. These grafts are best placed with this approach as it gives the control over graft length/tunnel mismatch (in case of BTB) and screw divergence (in fixation) directly in the hands of the surgeon
In a revision ACLR, where a previously drilled good tunnel is in place but cannot be used or where a tunnel is in a partially correct location, overlapping with the intended new tunnel, this technique is particularly useful, in that it allows us to retain the desired entry point, using a different trajectory.
While a femoral tunnel is routinely drilled outside-in by most colleagues in PCLR, the same is done infrequently in ACLR, where it is reserved for a revision scenario or while handling a multi- ligament injured knee to avoid tunnel coalescence.[3] When confronted with outside-in drilling in ACLR for the femoral tunnel, the surgeon may be mistaken into thinking that the same ease with which he/she is able to do it in PCLR will translate in this scenario. Outside-in femoral tunnel drilling in ACLR is more difficult than in PCLR for these reasons:
The femoral jig needs to be placed deep into the intercondylar notch and the standard anterolateral portal is too high and lateral to permit it’s accurate insertion
The arthroscope and the aiming arm of the jig compete for space in the tight confines of a standard intercondylar notch, as the placement becomes deeper [Figure 1]. This is made worse by the presence of an intact PCL and an ACL stump in most instances. This is unlike the situation in PCLR, wherein the jig is placed in a shallow location on the medial femoral condyle, permitting enough room for all round visualization by the arthroscope, which occupies the much roomier portion of the anterolateral joint space [Figure 2].
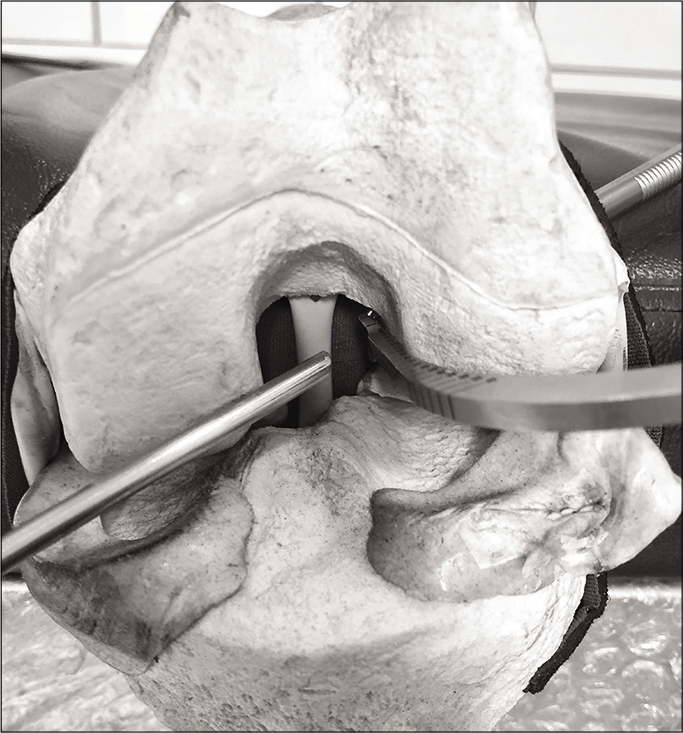
- Deep placement of femoral jig leads to frequent clashes with the scope in the tight space of intercondylar notch in anterior cruciate ligament reconstruction.
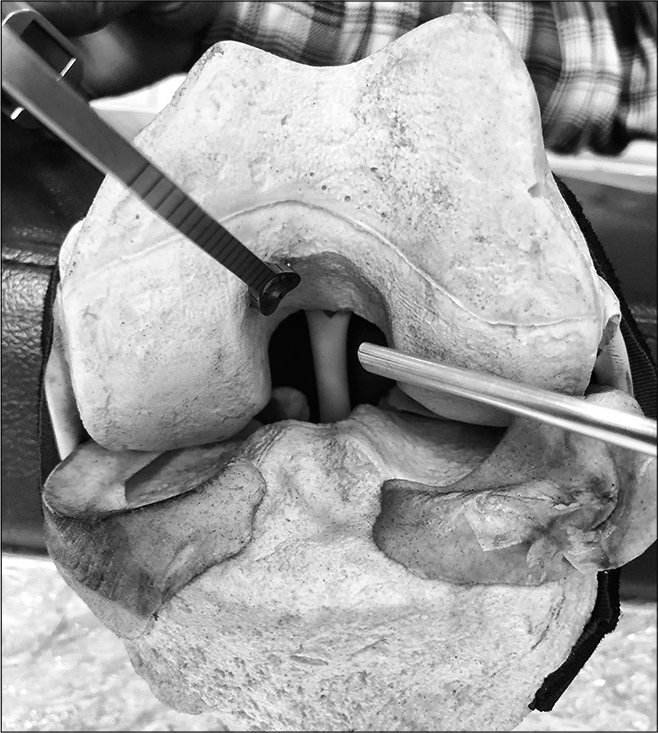
- Jig placement, handling and visualization are relatively easier in posterior cruciate ligament reconstruction due to the shallow placement in the notch.
This tricky situation leads to inadequate visualization of the tip of the aiming arm of the outside-in jig as it is placed deeper in the notch, due to frequent scope-jig collisions, thereby compromising the placement of the femoral guide wire in ACLR. This paper describes a simple and reproducible technique to place the guide wire correctly and consistently, while drilling the femoral tunnel in ACLR outside-in, by building on the established techniques for the same in the inside-out manner. This works best with bull’s eye aiming jigs [Figure 3] and with a steady hand can also work equally well with tip aiming jigs.
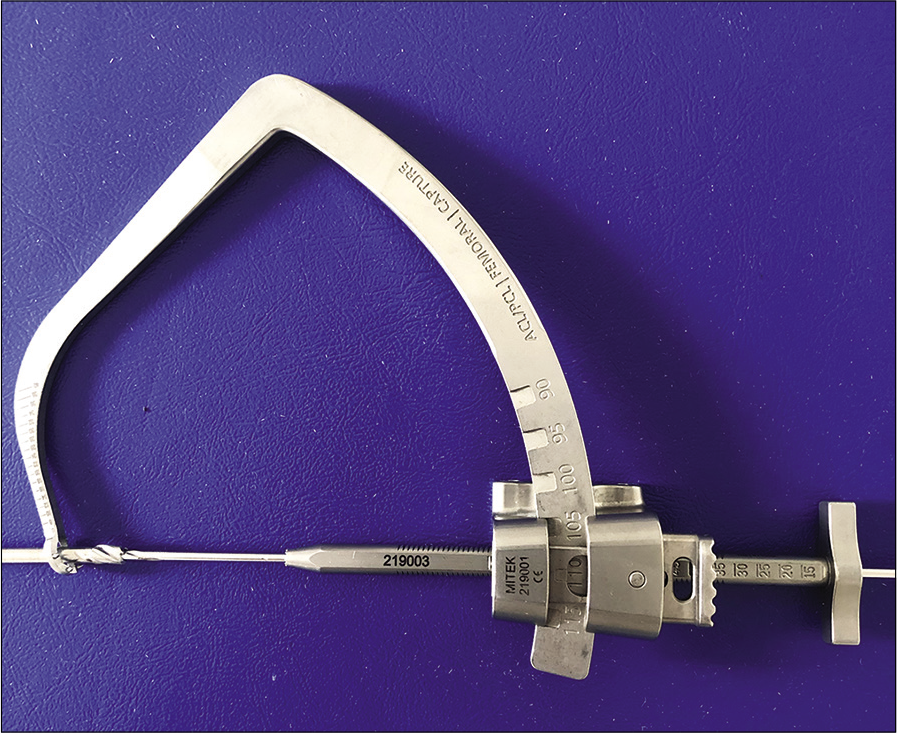
- Standard outside-in femoral jig.
SURGICAL TECHNIQUE
Positioning and anesthesia
Standard supine positioning with a lateral post and flexion stop to hold the knee in 90 degree flexion are employed. The most appropriate anesthesia is spinal anesthesia combined with a 3 in 1 block for post-operative pain relief.
Graft
This technique can be used with any graft, though I prefer to use the BTB and CQT with patellar bone plug while doing this technique.
Technique Pearls [Video 1]
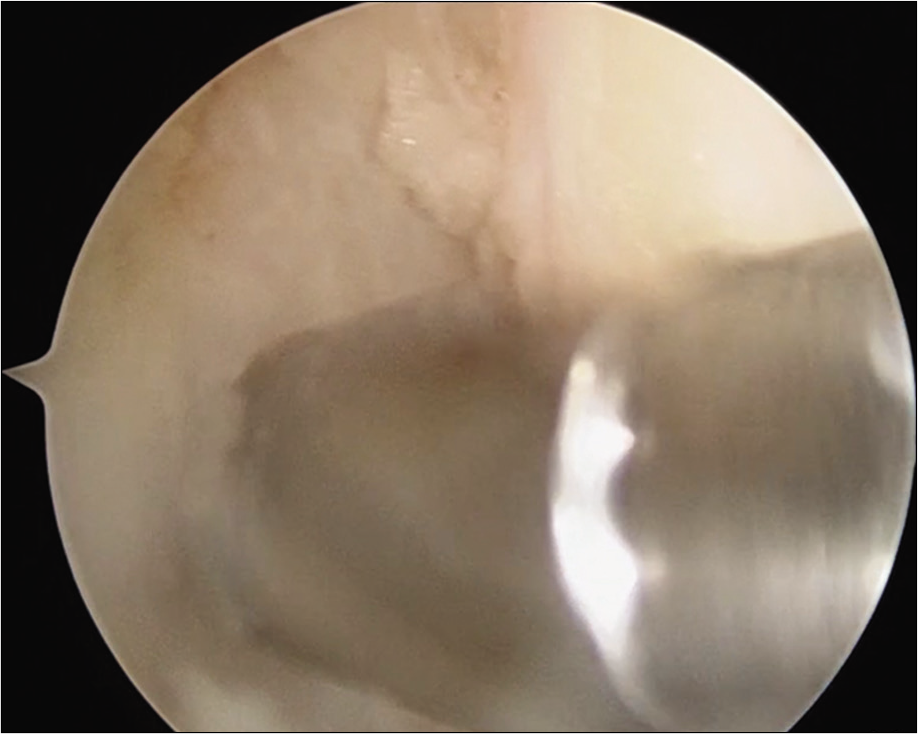
Use a microfracture awl to create a pilot hole as you would in a standard inside out technique with the knee in 90 degree flexion [Figure 4]. One could also take the assistance of a medial portal offset jig in doing so
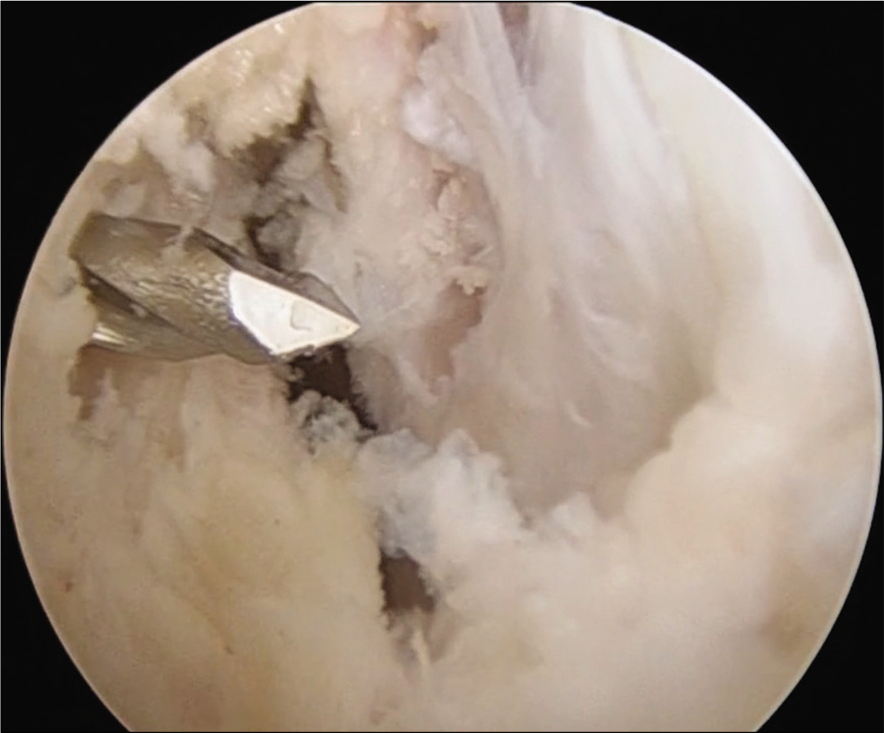
Drill a 2.4 mm beath pin for 20–30 mm into the previously made hole [Figure 5]
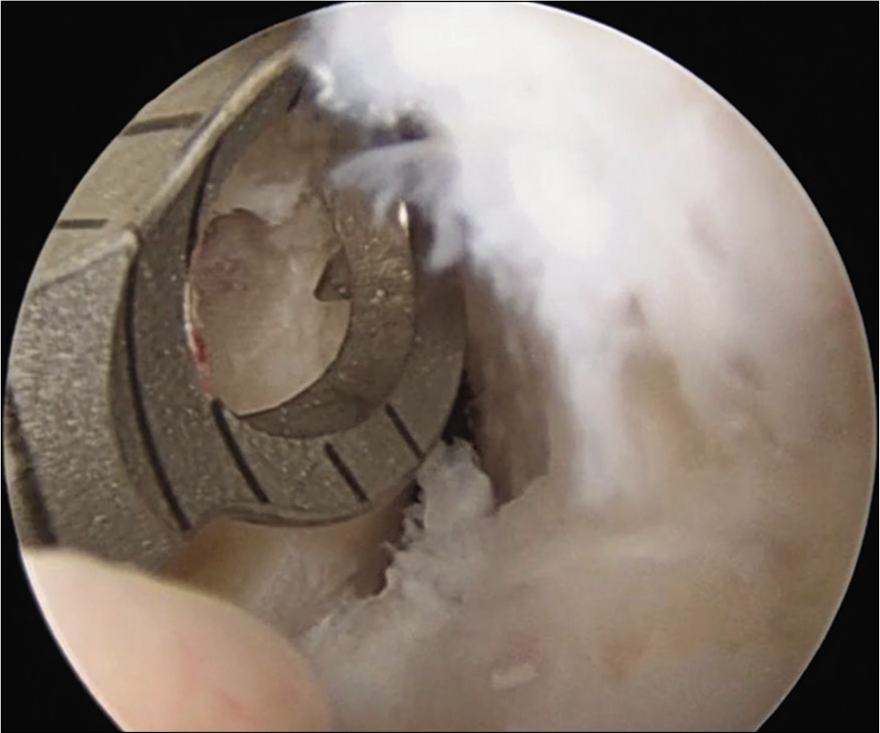
Ream this beath pin with a 4.5/4.7 mm reamer for 20–30 mm [Figure 6]. Ensure that you do not come out of the lateral cortex of the femur to prevent stress risers
In most instances, an accessory lateral portal is made with the guidance of a spinal needle, at the lateral edge of the patellar tendon, to ensure collinearity with the medial wall of the lateral femoral condyle so that the jig is not deflected medially off the condylar contours. In case BTB, graft is harvested, the jig is best placed through the central tendon defect
Ensure that there is overlap of the jig’s eye with the previously created hole [Figure 7] in the femoral wall and proceed with standard outside in guide-wire placement [Figure 8]
The external placement of the bullet is under the surgeon’s direct control. The jig is usually set at an angle of 55 degrees and a small dimple is created in the skin of the distal lateral thigh roughly in the mid-coronal plane, near the lateral epicondyle. Dissection is carried out sharply after splitting the ITB directly onto the lateral femoral cortex
In case, a LET is also planned, this incision may be made beforehand to harvest the ITB strip as described in the literature.[4] The resultant defect may be utilized to place the bullet for the outside-in guide wire
The surgery is then completed in a standard manner as may be the case depending on the graft and final fixation [Figure 9].
Video 1:
Video 1:Technique video demonstrating femoral guide wire placement using an outside-in jig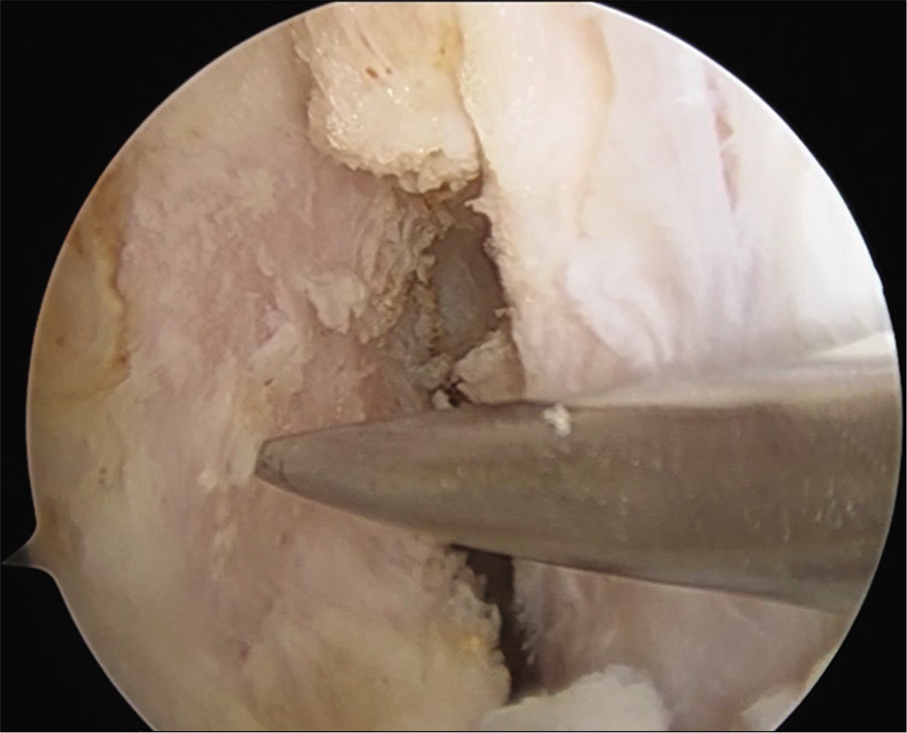
- Creating a pilot hole using an awl.

- Drilling a beath pin into the pilot hole.
- Creating a footprint with the 4.5/4.7 mm reamer.
- Ensuring that the jig correctly overlaps the drilled footprint.
- Femoral guide wire drilled correctly.
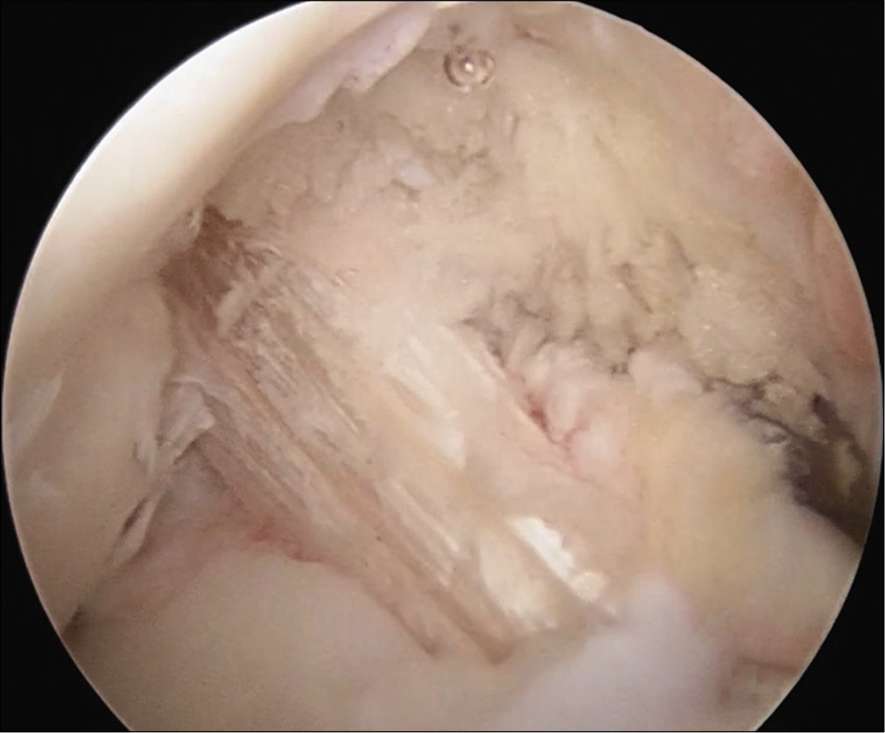
- Final picture showing the graft (CQT) in place.
Pitfalls
Ensure adequate knee flexion/hyperflexion while drilling the beath pin to prevent the wire/reamer blowing the posterior femoral cortex
Ream/drill only to a depth of 20–30 mm, do not breach lateral cortex to prevent stress risers
Always verify pilot hole placement from medial portal
Do not hesitate to create additional portals for better jig trajectory
Ensure jig portal is generous and adequately dilated with a hemostat, use a small cannula if necessary to prevent struggle with the fat pad.
CONCLUSION
Pre-determining the femoral entry point in a standard inside-out manner eliminates most of the difficulty and guesswork while drilling outside-in for the femoral tunnel in ACLR.
Combining LET (modified Lemaire) with ACLR converts the only disadvantage of outside-in drilling, namely, the need to give an additional lateral incision into a strategic advantage.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Video available on:
References
- The ability of 3 different approaches to restore the anatomic anteromedial bundle femoral insertion site during anatomic anterior cruciate ligament reconstruction. Arthroscopy. 2011;27:200-6.
- [CrossRef] [PubMed] [Google Scholar]
- One-incision versus two-incision techniques for arthroscopically assisted anterior cruciate ligament reconstruction in adults. Cochrane Database Syst Rev. 2017;12:CD010875.
- [CrossRef] [PubMed] [Google Scholar]
- Anterior cruciate ligament femoral tunnel length: Cadaveric analysis comparing anteromedial portal versus outside-in technique. Arthroscopy. 2010;26:1357-62.
- [CrossRef] [PubMed] [Google Scholar]
- Modified lemaire lateral extra-articular tenodesis augmentation of anterior cruciate ligament reconstruction. JBJS Essent Surg Tech. 2019;9:e41.1-7.
- [CrossRef] [PubMed] [Google Scholar]




